
Translate this page into:
Mandibular function and differential diagnosis of restricted mouth opening

*Corresponding author: T. Rathiya, Intern, Department of Oral and Maxillofacial Surgery, Government Dental College and Hospital, Cuddalore, Tamil Nadu, India. rathiyathangavel@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Rathiya T, Thangavelu A, Laxmi RB. Mandibular function and differential diagnosis of restricted mouth opening. J Academy Dent Educ. 2025;11:71-5. doi: 10.25259/JADE_99_2023
Abstract
The mandible is a unique bone as it is the largest and only movable bone in the human skull. It holds the lower teeth in place; it assists in mastication and forms the lower jawline. It enables various movements essential for eating and speaking, including opening and closing the mouth and moving the jaw from side to side. Any defect in relevant anatomic structures such as temporomandibular joint (TMJ), muscles, and tongue that disturbs the free physiological movement of the jaw might result in restricted mouth opening (trismus). Every practicing dental surgeon should know that any abnormal conditions of surrounding anatomical structures that disturb mandibular function might cause restricted mouth opening. The outcome of this abnormality is critically dependent on timely diagnosis and treatment, and it is difficult to identify the true origin in some cases. In this article, we discuss about the various causes of restricted mouth opening, starting from pediatric TMJ ankylosis, fracture of the mandible, and carcinoma of the oral cavity. Surgeons should remain vigilant to the possibility of restricted mouth opening from any abnormal condition relevant to anatomic structures.
Keywords
Ankylosis
Mandibular fracture
Temporomandibular joint
Trauma
Trismus

INTRODUCTION
The facial skeleton has movable and immovable bones. They protect the vital structures present within it and aids in other functions. The mandible is unique as it is the largest and only movable bone in a human skull. Mandibular functions are opening, closing, retraction, rotation, protrusion, lateral movements, mastication, swallowing, and speaking. Various muscles, joints, soft tissues, etc., altogether contribute to mandibular functions. If there is any abnormality in these structures, the mandibular functions are affected. Every dentist should know the conditions associated with restricted mouth opening (trismus), which could be attributed to various reasons such as; in case of joint – temporomandibular joint ankylosis; soft tissue–oral submucous fibrosis, carcinoma; and skeletal – fractures, large tumors. Restricted mouth opening has a detrimental effect on quality of life. The following Image 1 shows us the classification of various causes of restricted mouth opening.
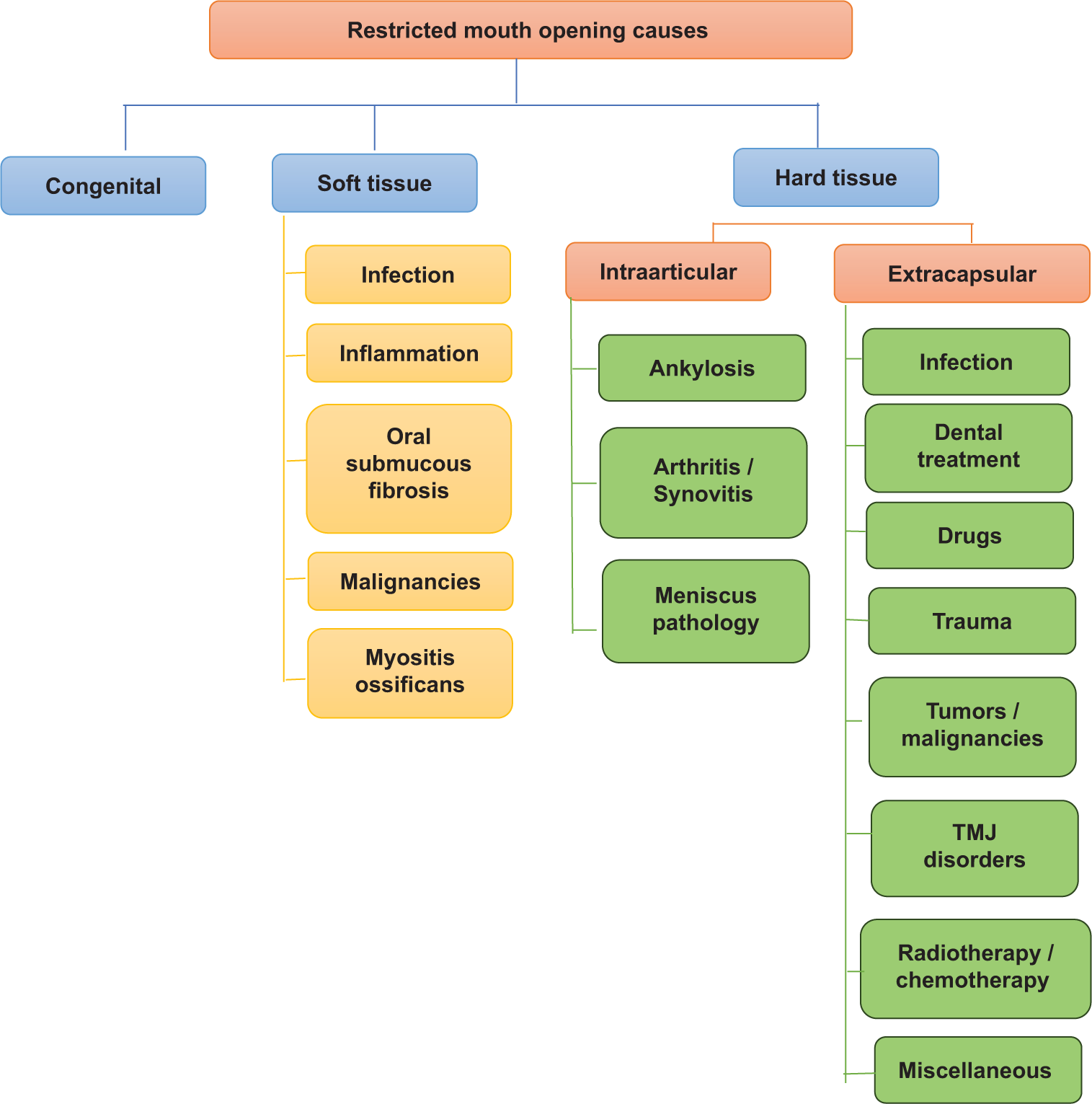
- Classification of causes of restricted mouth opening. TMJ: Temporomandibular joint.
CASE SERIES
Case 1
A 12-year-old female child reported to the Department Oral and Maxillofacial Surgery (OMFS), Government Dental College and Hospital, Cuddalore District with a chief complaint of difficulty in mouth opening [Figure 1a] for past 8 years. Patient’s attenders gave a history of fall injury of the patient from bed when she was 2 years old and sustained an injury over her chin. Since then, the mouth opening for the patient has decreased gradually. She did not have any associated medical or surgical history. On clinical examination, it was revealed that the patient did not have any significant facial asymmetry but a convex profile and retruded chin, condyle was not palpable on the left side. On radiographic examination [Figure 1b], orthopantomogram revealed a huge condylar notch to the condylar fossa and reduced joint space in the left side temporomandibular joint (TMJ), reduced Ramal height on the left side, antegonial notch, and a radio-opaque mass over the left TMJ leading to the diagnosis of the left TMJ ankylosis.
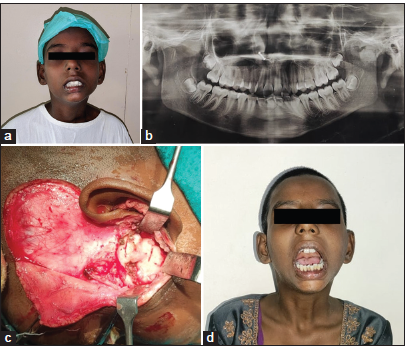
- Case 1 (a) Pre-operative profile picture, (b) Pre-operative radiograph, (c) Intra operative image of condylectomy, and (d) Post-operative profile picture.
The patient was planned for release of left TMJ ankylosis according to Kaban’s protocol, with ipsilateral condylectomy [Figure 1c] and coronoidectomy followed by interposition with free fat dermis under general anesthesia (GA). Consent for surgery was obtained from the parents and patient. Mouth opening was improved from 2 mm preoperatively to 25 mm postoperatively after 1 year of follow-up [Figure 1d].
Case 2
A 33-year-old female patient came to the department with a chief complaint of difficulty and pain while mouth [Figure 2a] followed by a road traffic accident. She was primarily treated in Cuddalore Medical College and Hospital Casualty and admitted in OMFS ward for further management. The patient’s general health status was normal. Based on clinical and radiographic examination, she was diagnosed with a fracture of the right parasymphysis and fracture of the left subcondyle [Figure 2b]. Upper and lower arch bar were placed under local anesthesia and intermaxillary fixation (IMF) was done.
She was planned for open reduction with internal fixation (ORIF) under GA over the fractured site [Figure 2c]. Postoperatively, her mouth opening was improved from 10 mm to 38 mm, and she was able to perform lateral protrusive movements with no other complaints [Figure 2d].
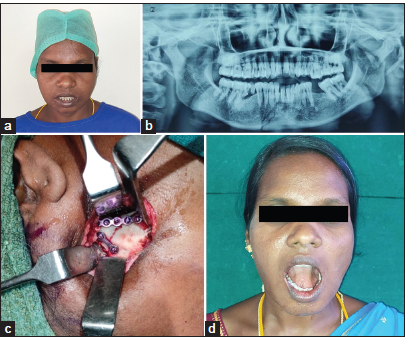
- Case 2 (a) Pre-operative profile picture, (b) Pre-operative radiograph, (c) Intra-operative image of internal fixation, and (d) Post-operative profile picture.
Case 3
A 69-year-old male patient had come to the department with a chief complaint of reduced mouth opening (8 mm) for the past 3 months [Figure 3a]. The patient was normal a few months back but later developed a progressive decrease in mouth opening. The patient had a habit of chewing betel nut and tobacco for the past 45 years with a frequency of 3–4 times a day. No previous medical and surgical intervention was done. On examination, it was revealed that the patient had bilateral vertical bands on the buccal mucosa and he also had suspected malignant growth; incisional biopsy was done from the left buccal mucosa, which was revealed to be squamous cell carcinoma.

- Case 3 (a) Pre-operative profile picture, (b) Intra-operative image of surgical excision, (c) Intra-operative image of nasolabial flap, and (d) Post-operative profile picture.
Under GA, wide local excision [Figure 3b] and reconstruction with local nasolabial flap [Figure 3c] was done. The immediate post-operative mouth opening was 22 mm [Figure 3d]. The patient was followed up for every 2 weeks for the 1st 2 months and later once every month.
DISCUSSION
The term “trismus” has been used to describe any restrictions to mouth opening, including restrictions caused by infection, trauma, surgery, or radiation. (Johnson et al, 2012).[1] Multiple conditions could lead to trismus, such as trauma, temporomandibular disorders, neoplasms, radiation, and connective tissue disorders and infections. Apart from these etiologies other factors such as pericoronitis, dentoalveolar abscess or infection should be considered for differential diagnosis of trismus. To narrow down the cause of trismus, a detailed history and physical examination are essential. This might include evaluating recent dental work, trauma history, and associated symptoms such as pain, swelling, or systemic illness. Imaging studies and laboratory tests can also provide additional information to aid in diagnosis.
Difficulty in mouth opening can be categorized due to soft tissue, hard tissue, and intra-articular and extracapsular causes.
Infections, chewing habits, could cause reduced mouth opening or trismus involving the soft tissues such as myositis and muscular spasms. Infections could be of dental origin, such as dental caries or periodontal, which could lead to space infections involving the muscles of mastication, such the masseter or it could be of non-dental origin such as tonsillitis or parotitis, one should be able to differentiate both. These conditions can be managed conservatively with the use of medical and physiotherapy, and severe cases could be managed by a surgical intervention such as wide local excision and reconstruction with local flaps. If the trismus (true trismus) is due to hard-tissue involvement, such as in case of TMJ, ankylosis/fracture of the mandible has to be treated with release of ankylosis and appropriate reconstruction depending on age and severity of ankylosis. Fracture of mandible leads to deranged occlusion and restricted mouth opening, often leading to facial asymmetry. ORIF has been done for fractured mandible to maintain the anatomy and, hence, increase the function, that is, the occlusion. Sometimes even fracture of zygomaticomaxillary complex or isolated zygomatic arch fracture can lead to restricted mouth opening by impeding the movement of the coronoid process. Cases of misdiagnosis of trismus as temporomandibular disorder leading to delayed diagnosis of malignancy has been described in the literature. If a patient presents with any of the following signs and symptoms such as mouth opening <15 mm, no associated clicking sounds, lymphadenopathy, and intraoral soft-tissue lesion; further, radiographs have to be taken and referral to a senior clinician must be considered.[2-4]
In this paper, we have recorded patients with difficulty in mouth opening due to various causes such as neoplasm of soft-tissue origin, TMJ ankylosis, and fracture of mandible, each of which has been treated according to their causative factors. The management and approach should be individualized based on the specific cause and the severity of trismus. Treatment options ranges from conservative measures such as physiotherapy, and medications for milder cases to more specialized interventions for severe cases such as TMJ ankylosis. It is essential for the dental professional to have adequate knowledge regarding physiology and pathology of mouth opening for proper diagnosis and treatment plan and should be able to consult with an oral and maxillofacial surgeon to determine the most appropriate management strategy. The ultimate goal is to improve the jaw mobility, elevate discomfort, and enhance the patient’s quality of life.
Review of literature
Clinical and retrospective study by Zhou et al., in 2018, mentioned that in case of maxillofacial fractures, patients having severe restricted mouth opening has to undergo surgical management and those who have no proper occlusion or mild-to-moderate mouth opening may prefer a non-surgical management.[5]
Prospective study by Boljevic et al., in 2019, mentioned that the amount of post-operative pain and trismus has positive relationship with difficulties that occur after internal rigid fixation of mandibular corpus fractures.[6]
Clinical study by Park et al., in 2019, mentioned that the surgical excision of the whole ankylosed mass and postoperatively aggressive physiotherapy are required in the management of TMJ ankylosis.[7]
Case report by starch – Jensen et al., in 2017, mentioned that the clinical and radiographic appearance of mandibular condylar process hyperplasia and elongated coronoid process, which impinges on the medial surface of the zygomatic arch is positively related to reduce mouth opening.[8]
Systematic review by Gondivkar et al., in 2020, mentioned that the regular use of devices for mouth exercise appeared to be effective in reducing restricted mouth opening in OSMF patients.[9]
Clinical review by Van der Geer et al., in 2020, mentioned that in cancer of head and neck, if a patient has large tumor approximating muscles of mastication or TMJ, which is most likely to cause reduced mouth opening. The first 6 months of the post-treat mental period of cancerous lesions are prone to restricted mouth opening.[10]
CONCLUSION
Trismus is a condition characterized by the restricted opening of the mouth due to muscle spasm, trauma, or other underlying causes. Its management and prognosis depend on identifying and treating the root cause, whether it is an infection, temporomandibular joint disorder, or other factors. Early diagnosis and appropriate intervention are crucial in preventing long-term complications and improving the quality of life for affected individuals. Treatment often involves a combination of physical therapy, medication, and in some cases, surgical intervention. Effective management also includes patient education on the importance of adherence to therapeutic exercises and ongoing monitoring by health-care professionals to ensure optimal outcomes.
Acknowledgement
Authors admit our heartfelt thanks for the persistent support from our optimistic, positive, and inspiring Prof. Dr. Annamalai Thangavelu MDS Sir. Really, we felt gratified to publish the article under your precious guidance.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Development and validation of the Gothenburg Trismus Questionnaire (GTQ) Oral Oncol. 2012;48:730-6.
- [CrossRef] [PubMed] [Google Scholar]
- Research achievements of oral submucous fibrosis: Progress and prospect. Biomed Res Int. 2021;2021:6631856.
- [CrossRef] [PubMed] [Google Scholar]
- Unusual causes of reduced mouth opening and it's suitable surgical management: Our experience. Natl J Maxillofac Surg. 2010;1:86-90.
- [CrossRef] [PubMed] [Google Scholar]
- Trismus following different treatment modalities for head and neck cancer: A systematic review of subjective measures. Eur Arch Otorhinolaryngol. 2017;274:2695-707.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical, retrospective case-control study on the mechanics of obstacle in mouth opening and malocclusion in patients with maxillofacial fractures. Sci Rep. 2018;8:7724.
- [CrossRef] [PubMed] [Google Scholar]
- The quality of life of patients with surgically treated mandibular fractures and the relationship of the posttraumatic pain and trismus with the postoperative complications: A prospective study. Medicina (Kaunas). 2019;55:109.
- [CrossRef] [PubMed] [Google Scholar]
- Gap arthroplasty with active mouth opening exercises using an interocclusal splint in temporomandibular joint ankylosis patients. Maxillofac Plast Reconstr Surg. 2019;41:18.
- [CrossRef] [PubMed] [Google Scholar]
- Bilateral elongated mandibular coronoid process and restricted mouth opening: A case report. Open Dent J. 2017;11:670-8.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical efficacy of mouth exercising devices in oral submucous fibrosis: A Systematic review. J Oral Biol Craniofac Res. 2020;10:315-20.
- [CrossRef] [PubMed] [Google Scholar]
- Prognostic factors associated with a restricted mouth opening (trismus) in patients with head and neck cancer: Systematic review. Head Neck. 2020;42:2696-721.
- [CrossRef] [PubMed] [Google Scholar]




