
Translate this page into:
Impact of smoking on oral cavity by comparing carbon monoxide and carboxyhemoglobin levels with salivary pH in smokers of Salem district

*Corresponding author: S. R. Apoorva, Intern, Department of Oral Pathology and Oral Microbiology, Vinayaka Mission’s Sankarachariyar Dental College, Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamil Nadu, India. apoodheez10@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Apoorva SR, Jacob M, Fenn SM. Impact of smoking on oral cavity by comparing carbon monoxide and carboxyhemoglobin levels with salivary pH in smokers of Salem district. J Acad Dent Educ 2022;8:45-50.
Abstract
Objective:
Saliva is the first biological fluid exposed to the smoke and other contents of the cigar, which can cause structural and functional changes in saliva. Salivary pH is an important biomarker for detecting oral diseases. Cigarette smoke contains many toxic gases, of which, carbon monoxide (CO), plays a deleterious role in causing systemic illness in a person. As a result, a measure of exhaled CO (eCO), similar to exhaled Nitric Oxide, has been evaluated as a potential breath biomarker to detect smoking status and validate smoking cessation to prevent other systemic defects caused by smoking. The present study would investigate the effect of CO and carboxyhemoglobin (HbCO%) on the pH of the oral cavity of individuals with smoked tobacco habit.
Materials and Methods:
For this study, 60 male patients aged 18–55 years with smoking habit of a minimum of two cigarettes or beedis per day for a minimum period of one year reporting to the Department of Oral Medicine and Radiology were divided based on their smoking habit and type of smoked tobacco into two groups with each group consisting of 30 participants. To determine the eCO levels and HbCO% levels, a breath analyzer (piCOTM Smokerlyzer®) was used. Patients were asked to hold their breath for 15 s, place their lips tightly around the mouthpiece of the breath analyzer, and gently exhale through the mouthpiece as long as possible. CO levels in exhaled breath (eCO) in parts per million and HbCO% in the percentage of red blood cells carrying CO (HbCO%) were displayed on the display monitor. A digital pH meter was used to calculate the salivary pH from unstimulated saliva samples. The salivary pH readings, along with the eCO and HbCO%, were recorded in the tabular column for each patient.
Results:
In the present study, the cigarette smokers had a higher mean value of eCO levels. Similarly, cigarette smokers had higher mean HbCo% levels than beedi smokers. It was also observed that salivary pH of smokers was found to be altered when compared to non-smokers.
Conclusion:
The current study found that the level of CO in exhaled breath correlates with the HbCO% present in the blood, alerting tobacco users to the hidden fatality and therefore serving as an indicator in tobacco cessation programs to raise awareness of the effects of smoking on oral health. Furthermore, along with CO levels the pH of saliva was altered, demonstrating the dangers of tobacco and its products.
Keywords
Smoking
Smoked tobacco
Carbon monoxide
Carboxyhemoglobin
Salivary pH
Smoking cessation

INTRODUCTION
Over the years, tobacco has gained popularity and its use is apparently on hike despite various dreadful health hazards. With the snuff and puff form of tobacco ruling the minds of people, quitting such habits ultimately ends up being a tough choice, highly addictive due to the presence of stimulant nicotine, as the name suggests it has been derived from the plant nicotinia. This poses a big challenge to the medical and dental professionals as they find it difficult to convince the general public to quit smoking or curb the use of tobacco products. Numerous research works in different countries have emphasized possible hazardous effects of its use in whatever form it is used.
One of the known victims of the deadly use of tobacco, apart from the respiratory and cardiovascular systems, is the oral cavity. Tobacco products are the most potent carcinogens of all time. Saliva plays a crucial role in maintaining the oral health and what comes to light is that it is the first biological fluid that is exposed to the smoke and other contents of cigar which can cause structural and functional changes in saliva. The pH of saliva is an important biomarker to detect oral diseases.[1]
The smoke exhaled from cigarettes contains many toxic gases, of which the most common topic of interest – carbon monoxide (CO) plays a deadly role in causing systemic illness in a person. Hence, the measure of exhaled CO (eCO) similar to exhaled nitric oxide has been evaluated as a candidate breath biomarker both to detect the smoking status and to validate smoking cessation so that other systemic defects due to smoking are prevented. Breath analyzer determines the presence of harmful by products like CO quantifying both abnormal respiration and oxygen levels in the blood.[2-6] The exposed values show the status of respiratory function and condition in the patients. One of the major advantages of the device is that it is simple to use and non-invasive, assuring of patient compliance. Approximate levels of carbon monoxide was found out to be around 400 parts per million (ppm) in a chronic smoker.[7,8]
Many studies have reported that the presence of carbon monoxide in the blood of smokers helps in the estimation of both the habit and its cessation in them. To minimize the consumption of various tobacco products, the government has enforced various measures, of which, the tobacco cessation centers, providing free counseling, and tobacco substitutes are noteworthy. Apart from this, social media and newspaper, magazines play a pivotal role in public awareness campaigns against the use of tobacco products.[9-11]
The present study would investigate the effect of CO and carboxyhemoglobin (HbCO%) levels on the pH of the oral cavity of individuals with smoked tobacco habit.
MATERIAL AND METHODS
Ethical committee approval
This study was carried out following approval from the Institutional Ethics Committee (IECApproval No.270).
Study design
This is a cross-sectional type of study with a sample size of 60 participants among the smoking population of Salem district and random sampling was applied. The participants were categorized into two groups of 30 each with the Group I consisting of Beedi/Cigarette smokers and Group II of 30 non-smokers as the control subjects.
Study groups
For this study, 60 male patients aged between 18 and 55 years reporting to the Department of Oral Medicine and Radiology were included in the study. Case history and informed consent were obtained from all patients before sample collection. Participants were classified into two groups with each group consisting of 30 participants, based on the habit of smoking and type of smoked tobacco used [Table 1].
| Cigarette smokers | 30 |
| Beedi smokers | |
| Non-smokers (control subjects) | 30 |
Selection criteria
For Group I, male patients with the habit of smoking a minimum of 2 cigarettes or beedis for a minimum period of 1 year were included and for Group II, male patients with no habit of tobacco usage were included in the study.
Exclusion criteria
Female patients were excluded from the study. Male patients with <1 year of smoking habit and using multiple tobacco products were excluded from the study. Patients who had used mouth wash on the day of reporting to the dental OP were also excluded from the study.
Determination of eCO levels and HbCO% levels
The patients were instructed not to smoke for at least 3 h before the experiment. Before the procedure, the participants were taken to the sample collection room in the department and briefed on the steps involved in obtaining the reading. The participants’ exhaled breath samples were collected using the breath analyzer (piCOTM Smokerlyzer®) available in the Department of Oral Medicine and Radiology. Participants were instructed to hold their breath for 15 s, place their lips tightly around the mouthpiece of the breath analyzer, and exhale as gently as possible through the mouthpiece. The participants were told not to forcefully expel their breath as this would displace the valve pin [Figure 1]. When necessary, the test was repeated after the display monitor was reset. CO levels in exhaled breath (eCO) in ppm and HbCO% in the percentage of red blood cells carrying CO (HbCO%) were displayed on the display monitor [Figure 2]. Each patient’s eCO and HbCO% readings were recorded in a tabular column.

- Sample of the participants exhaling through the breath analyzer.
- Sample of the reading from the display monitor of breath analyzer.
Determination of salivary pH
Participants were instructed to spit 1.5 mL of unstimulated saliva into sterile sample collection containers to estimate salivary pH. The participants’ saliva was collected in a sterile container between 9 a.m. and 12 p.m., and the pH was estimated using the Central Research Laboratory’s pH Meter (Deep Vision, Deluxe pH Meter, Model - 101). The collected sample was taken directly (within 10 min) to the Central Research Laboratory, where the pH of the saliva was determined using a digital pH meter [Figure 3]. The digital pH meter’s accuracy was checked on a regular basis to ensure accurate readings. The salivary pH readings for each patient were recorded in the tabular column alongside the eCO and HbCO%.

- pH meter (Deep Vision, Deluxe pH Meter, Model-101).
Statistical analysis
The obtained values of eCO, HbCO% and salivary pH of the participants from the two groups were entered into an MS Excel sheet as shown in [Figure 4] and the data were analyzed using SPSS software applying the statistical analyses, ANOVA, and correlation analyses.
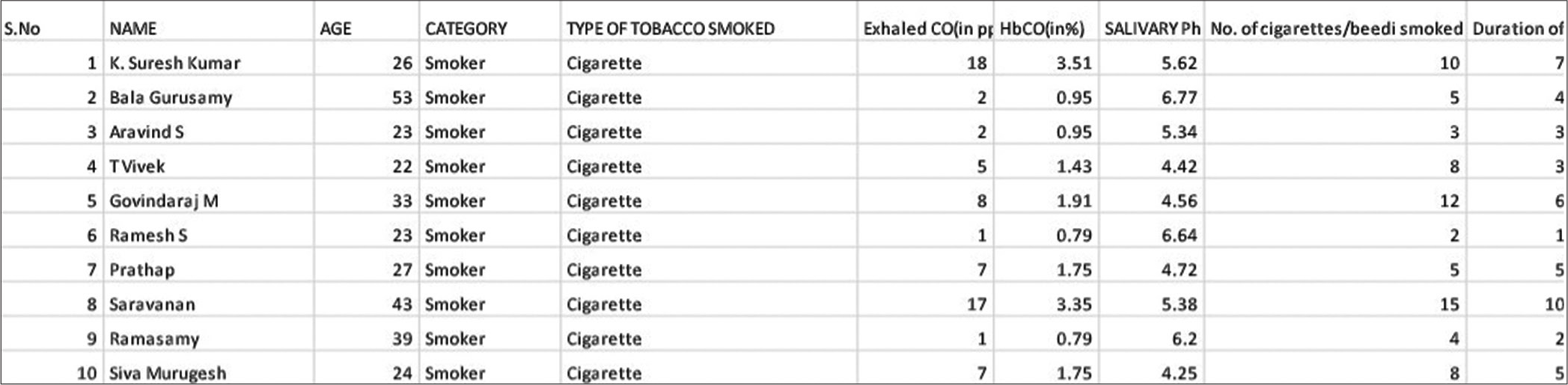
- Sample of recording format of exhaled carbon monoxide, carboxyhemoglobin, and salivary pH of the study participants.
RESULTS
Results of the analysis on distribution of study participants based on age, number of cigarettes or beedis smoked per day, and duration of smoking gives the mean value of the age if the study participants as 29.02 with the minimum age being 19 years to a maximum of 53 years. Results of the analysis give the mean value of the number of cigarettes/beedis smoked by the study participants as 2.68 with the minimum number being 0 (including a non-smoker) to a maximum of 15. Results of the analysis give the mean value of the duration of smoking by the study participants as 1.83 with the minimum of 0 years to a maximum of 10 years as shown in [Table 2].
| n | Minimum | Maximum | Mean | Std. Deviation | |
|---|---|---|---|---|---|
| Age | 60 | 19 | 53 | 29.02 | 8.003 |
| Type of tobacco smoked | 30 | 1 | 3 | 2.05 | 0.982 |
| No. of cigarettes/beedi smoked per day | 30 | 0 | 15 | 2.68 | 3.587 |
| Duration of smoking | 30 | 0 | 10 | 1.83 | 2.366 |
Results of the analysis on the distribution of study subjects based on the type of smoked tobacco used show that the mean value of eCO levels in smokers (both cigarette and beedi smokers) was found to be 5.96 while in the non-smokers it was found to be 0.73. Hence, a statistically significant difference in the eCO levels was observed between smokers and the non-smokers as shown in [Figure 5]. In addition to this, the eCO Levels in cigarette smokers was found to be 6.11 while it was found to be 4.67 in case of beedi smokers thereby showing a higher eCO levels in cigarette smokers than in beedi smokers. A statistically significant difference in eCO levels (P = 0.00) observed between cigarette smokers and beedi smokers as shown in [Table 3].
| Cigarette | ||||||
| Mean | 29.48 | 6.11 | 1.6078 | 6.1370 | 5.44 | 3.74 |
| Std. Deviation | 8.577 | 5.673 | 0.90763 | 2.07868 | 3.534 | 2.159 |
| Beedi | ||||||
| Mean | 37.67 | 4.67 | 1.3767 | 5.6200 | 4.67 | 3.00 |
| Std. Deviation | 5.132 | 3.786 | 0.60575 | 0.87023 | 0.577 | 1.732 |
| Nil | ||||||
| Mean | 27.73 | 0.73 | 0.5163 | 9.1723 | 0.00 | 0.00 |
| Std. Deviation | 7.273 | 0.640 | 0.40237 | 1.76735 | 0.000 | 0.000 |
| P-value | 0.112 | 0.000* | 0.000* | 0.000* | 0.000* | 0.000* |
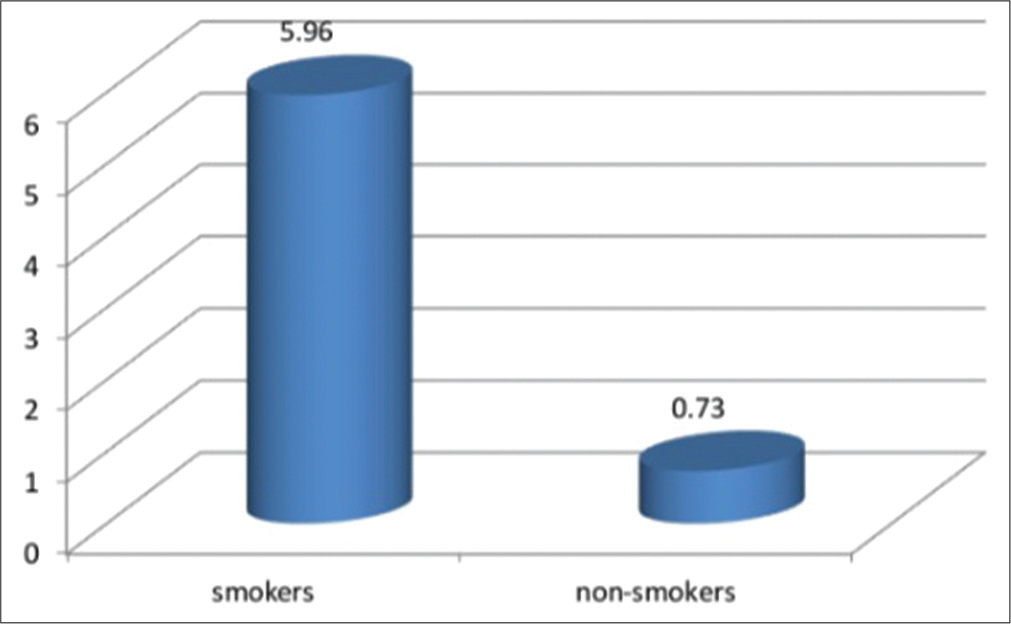
- Mean exhaled carbon monoxide levels of smokers and non-smokers.
Results of the analysis show that mean value of HbCO% levels in smokers (both cigarette and beedi smokers) was found to be 1.58 while in the non-smokers it was found to be 0.51. Hence, a statistically significant difference in the HbCO% levels was observed between smokers and the non-smokers as shown in [Figure 6]. In addition to this, the HbCO% levels in cigarette smokers was found to be 1.6 while it was found to be 1.37 in case of beedi smokers thereby showing a higher HbCO% levels in cigarette smokers than in beedi smokers. A statistically significant difference (P = 0.00) in HbCO% levels observed between cigarette smokers and beedi smokers as shown in [Table 3].
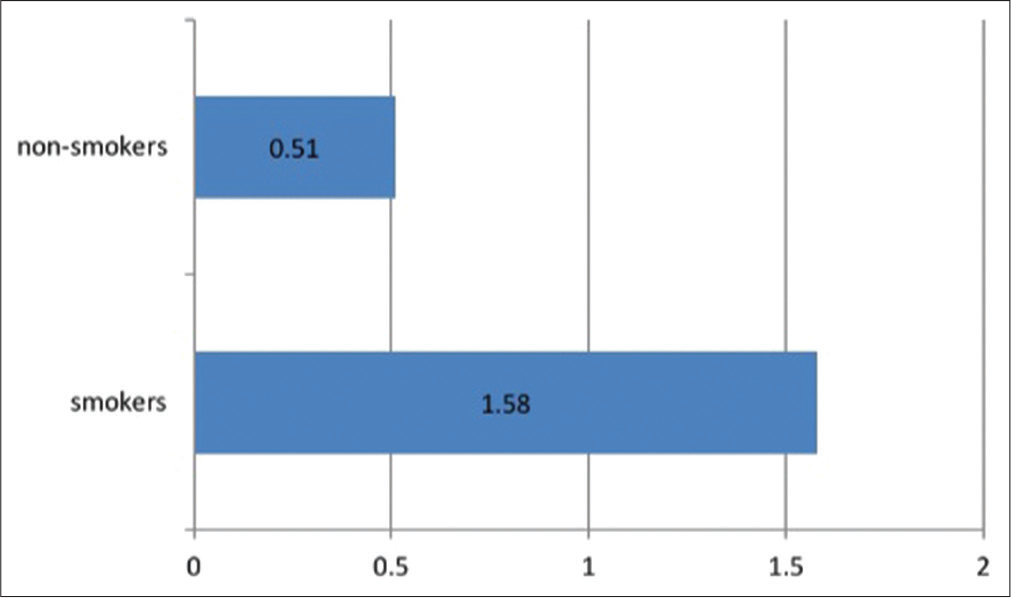
- Mean carboxyhemoglobin levels of smokers and non-smokers.
Results of the analysis show that mean salivary pH of smokers (both cigarette and beedi smokers) was found to be 6.08 while in the non-smokers it was found to be 9.17. Hence, a statistically significant difference in the salivary pH was observed between smokers and the non-smokers as shown in [Figure 7]. In addition to this, the salivary pH in cigarette smokers was found to be 6.13 while it was found to be 5.62 in case of beedi smokers thereby showing an even more acidic nature of saliva in beedi smokers than in cigarette smokers. A statistically significant difference in salivary pH (P = 0.00) observed between cigarette smokers and beedi smokers as shown in [Table 3].
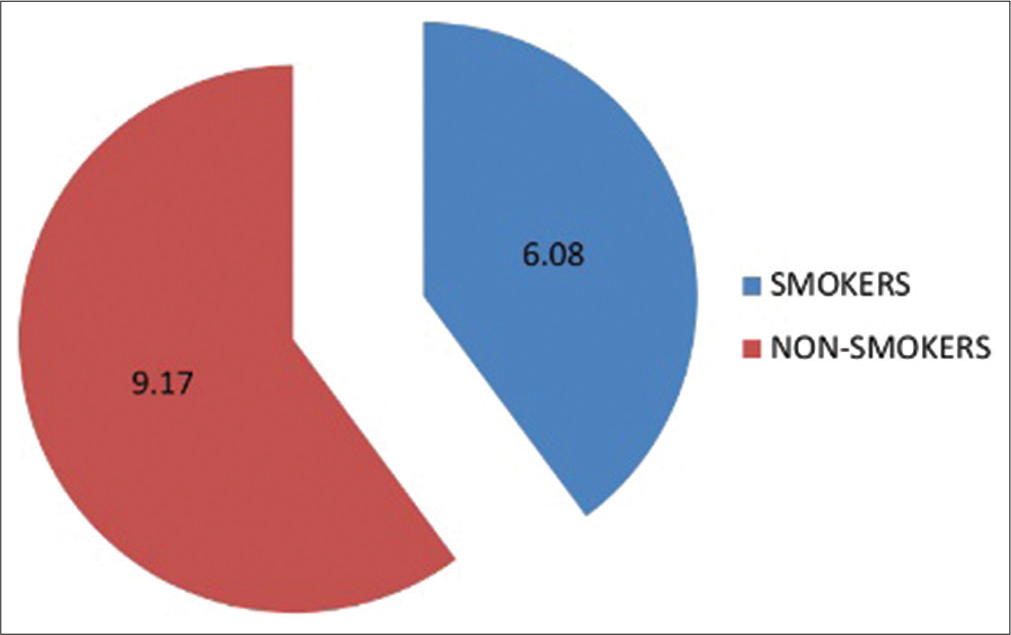
- Mean salivary pH levels of smokers and non-smokers.
Correlation results for Group I (smokers) and Group II (non-smokers) based on age, CO, HbCO%, salivary pH, and the type of tobacco smoked along with the quantity and duration. CO levels, HbCO% levels, and salivary pH were found to be positively correlated with the type of tobacco smoked, its quantity, and duration as shown in [Table 4].
| Age | |
| Pearson correlation | −0.110 |
| Sig. (2-tailed) | 0.402 |
| n | 60 |
| eCO (in ppm) | |
| Pearson correlation | −0.564** |
| Sig. (2-tailed) | 0.000 |
| n | 30 |
| HbCO (in %) | |
| Pearson correlation | −0.620** |
| Sig. (2-tailed) | 0.000 |
| n | 30 |
| Salivary pH | |
| Pearson correlation | 0.615** |
| Sig. (2-tailed) | 0.000 |
| n | 30 |
| No. of cigarettes/beedi smoked per day | |
| Pearson correlation | −0.746** |
| Sig. (2-tailed) | 0.000 |
| n | 30 |
| Duration of smoking | |
| Pearson correlation | −0.777** |
| Sig. (2-tailed) | 0.000 |
| n | 60 |
| Type of tobacco smoked | |
| Pearson correlation | 1** |
| Sig. (2-tailed) | |
| n | 30 |
eCO: Exhaled carbon monoxide, HbCO: Carboxyhemoglobin, **Negative correlation
DISCUSSION
The statistical analyses used in this study were to determine if the levels of eCO in breath and HbCO% levels in blood detected by the breath analyzer were comparable or different between smokers and non-smokers, and if there was a correlation between the levels. The study also revealed a significant difference in CO and HbCO% levels between smokers and non-smokers, implying that smokers are exposed to more CO than non-smokers.
Although tobacco and its products are widely regarded as stress relievers, long-term use can become addictive. Increased tobacco use, according to the study, can raise CO levels, which are absorbed by red blood cells after passing through the lungs. This raises the blood HbCO% level which corroborate with findings of similar research.[12] A normal level of HbCO%, the hemoglobin grouped with CO, in non-smokers is <1.5%. HbCO% levels in cigarette smokers can range from 3% to 15%. Because of the presence of unrefined and unfiltered contents in beedi, smoking beedi produces significantly more CO than smoking cigarettes. CO is not added to tobacco products, but it is produced as a by-product of partial combustion. This occurs when there is not enough oxygen to convert all of the carbon in the tobacco into a harmless form called carbon dioxide.
The current study also found that smokers had higher levels of HbCO% than non-smokers, with beedi users having higher levels than cigarette smokers. Cigarette smokers have a higher mean value of eCO and a higher percentage of HbCO%, indicating the presence of large amounts of CO in cigarette smoke, which has 245 times more affinity for hemoglobin than oxygen.[13] This information can be utilized by tobacco cessation centers to educate and encourage smokers to quit.
The current study also observed a positive relationship between CO, HbCO%, and the type of smoked tobacco used, revealing that when the consumption of cigarettes or beedis increases, the levels of CO, HbCO% rise not only in the breath but also in the blood.[14]
Saliva is required to maintain oral health by protecting the oral mucosa, remineralization of teeth, digestion, taste sensation, pH balance, and phonation.[15] The structure and function of saliva are altered by the contents of the cigar because it is the first biological fluid to be exposed to smoke. In the present study, the altered pH of saliva in smokers demonstrated that the major constituent of tobacco, nicotine, acts on some of the cholinergic receptors present in the brain and other organs stimulating the neurons which in turn alters the salivary secretion[16] In the present study, the altered pH of the smokers attribute to various harmful contents of the beedis or cigarettes smoked whereas in the non-smokers, the altered pH might be due to various other factors including the type of foods taken in by the participants during the study. Furthermore, as the current study used a smaller sample size of cigarette and beedi smokers, it was unable to correlate the effects of other tobacco products and alcohol with levels of carbon monoxide and HbCO% in patients who smoked and consumed alcohol in addition to using other tobacco products. As a result, for a more accurate analysis, additional research involving a larger population of both male and female patients with multiple tobacco consumption is required.
CONCLUSION
According to the findings of this study, beedi and cigarette smokers have significantly higher levels of CO and HbCO% than non-smokers. As the current study used a smaller sample size of cigarette and beedi smokers, further more research is required to derive accurate values. Moreover, in the study, the estimated salivary pH differs between smokers and non-smokers, that could be utilized in tobacco cessation programs to raise awareness about the effects of smoking on oral health.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Salivary pH: A diagnostic biomarker. J Indian Soc Periodontol. 2013;17:461-5.
- [CrossRef] [PubMed] [Google Scholar]
- Distribution of carboxyhaemoglobin concentrations in smokers and non-smokers. Thorax. 1986;41:25-7.
- [CrossRef] [PubMed] [Google Scholar]
- Blood carboxyhaemoglobin levels in Indian bidi and cigarette smokers. Respiration. 1991;58:26-8.
- [CrossRef] [PubMed] [Google Scholar]
- Carboxyhaemoglobin levels and inhaling habits in cigarette smokers. Thorax. 1978;33:201-6.
- [CrossRef] [PubMed] [Google Scholar]
- Carbon monoxide in breath in relation to smoking and carboxyhaemoglobin levels. Thorax. 1981;36:366-9.
- [CrossRef] [PubMed] [Google Scholar]
- Variations in carboxyhaemoglobin levels in smokers. Br Med J. 1974;4:736-8.
- [CrossRef] [PubMed] [Google Scholar]
- Carbon monoxide in exhaled breath testing and therapeutics. J Breath Res. 2013;7:1711.
- [CrossRef] [PubMed] [Google Scholar]
- Breath carbon monoxide concentration in cigarette and bidi smokers in India. Indian J Chest Dis Allied Sci. 2010;52:19-24.
- [Google Scholar]
- Quantification and chemical markers of tobacco-exposure. Eur J Respir Dis. 1987;70:1-7.
- [Google Scholar]
- Breath carbon monoxide as an indication of smoking habit. Chest. 2000;117:758-63.
- [CrossRef] [PubMed] [Google Scholar]
- Does breath carbon monoxide measure nicotine dependence? J Addict Dis. 2010;29:493-9.
- [CrossRef] [PubMed] [Google Scholar]
- What are the markers of tobacco smoking? J Gynecol Obstet Biol Reprod. 2005;34:154-70.
- [CrossRef] [Google Scholar]
- Correlation of smoking behaviour and blood carboxyhaemoglobin in bidi and cigarette smokers. Indian J Chest Dis Allied Sci. 1991;33:43-6.
- [Google Scholar]
- Carboxyhemoglobin levels induced by cigarette smoking outdoors in smokers. J Med Toxicol. 2018;14:68-73.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of smoking one cigarette on antioxidant metabolites in the saliva of healthy smokers. Arch Oral Biol. 1999;44:485-8.
- [CrossRef] [PubMed] [Google Scholar]
- Long-term effect of tobacco on unstimulated salivary pH. J Oral Maxillofac Pathol. 2016;20:16-9.
- [CrossRef] [PubMed] [Google Scholar]




