
Translate this page into:
Evaluating the staining effects of tobacco, oil, mouthwash, and beverages on teeth and restorative materials: A cross-sectional observational study

*Corresponding author: Mathew Jacob, Department of Oral Pathology and Oral Microbiology, Vinayaka Mission’s Sankarachariyar Dental College, Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamil Nadu, India. docere_mathew@yahoo.co.in
-
Received: ,
Accepted: ,
How to cite this article: Apoorva SR, Jacob M, Fenn SM, Rajathi P. Evaluating the staining effects of tobacco, oil, mouthwash, and beverages on teeth and restorative materials: A cross-sectional observational study. J Academy Dent Educ. 2024;10:64-70. doi: 10.25259/JADE_34_2023
Abstract
Objectives:
The purpose of this study was to examine the effect of water, mouthwash, coconut oil, coffee, tea powder, smoke, and smokeless tobacco on the dental hard tissue enamel of natural teeth and tooth-colored restorative materials.
Material and Methods:
The mediums included in the study were commercially available bottled water, mouthwash, oil and tobacco (both smoke and smokeless), coffee, and tea. M1–M8 was assigned to each medium. GIC and composite were used to fill cavities prepared on the labial and occlusal surfaces of anterior and posterior teeth, respectively. The teeth were divided into three groups: Natural (N), GIC filled (G), and composite filled (C) and were placed in the mediums for 24 h before being repeated consecutively for the next 6 days. Pre- and post-exposure photographs were taken before the first exposure and after the previous day exposure in the respective mediums. Following that, the four observers (blinded) were asked to rate the intensity of staining caused by the eight mediums on teeth and restorations.
Results:
Following the experiment, observations by the blind observers were recorded as positive and negative findings on the teeth preserved in the eight media. The positive findings, along with corresponding photographs were taken under a stereo zoom microscope. The present study revealed that chewable tobacco, tea, and coffee caused noticeable staining on the teeth and dental restorations compared to water, oil, and mouthwash.
Conclusion:
According to the findings of this study, exposure to smokeless tobacco, coffee, and tea caused staining on the hard tissue enamel of the crown and the cementum of the root. The clinical implications of this study are that patients must be educated about the increased susceptibility to staining of natural teeth, particularly in the exposed cementum of the cervical portion and tooth-colored restorations placed in anterior teeth.
Keywords
Dental stain
Intrinsic stain
Extrinsic stain
Tobacco products

INTRODUCTION
To meet the public’s growing desire for whiter teeth, new trends in esthetic dentistry have emerged, including tooth-colored restorative materials used as a substitute for traditional filling materials. Despite various advancements, tooth discoloration continues to be an issue not only on natural tooth surfaces but also on restored tooth surfaces. These discolorations due to stains can be caused by extrinsic stains, which occur as a result of staining by beverages, aerated drinks, or other foods, as well as prolonged smoking habits, or by intrinsic stains, which are seen in fluorosis or by excessive consumption of antibiotics such as amoxicillin/tetracycline, or by age-related issues that lead to tooth layer wear.[1-4]
The present study was conducted to determine the effect of extrinsic stains caused by the staining of water, rejuvenators such as tea and coffee, mouthwash, oil, and chewable and non-chewable tobacco products on the dental hard tissue enamel of natural teeth as well as teeth restored with tooth-colored restorative materials – glass-ionomer cement (GIC) and composites. As a result, this study may serve as a wake-up call for those who are unaware of the oral effects of their daily eating habits. It also aids in distinguishing the percentage of stains present in GIC and composite-restored teeth, providing insights into which material is superior for anterior restorations.
MATERIAL AND METHODS
Study setting
The study was carried out in the department of oral pathology and oral microbiology . The study was approved by the Institutional Ethics Committee on March 28, 2019 (Approval No. 124). All participants provided written informed consent for participation in the study. All procedures performed were conducted in accordance with the ethical standards set forth in the 1964 Declaration of Helsinki, as revised in 2013.
Study design
A cross-sectional study design was applied to the study.
Sample
Recently, extracted central incisors and premolars were collected from our dental college’s departments of oral surgery and orthodontics for this study. All of the collected teeth were cleaned with a toothbrush and toothpaste and stored in saline until the study. Each tooth’s root apex was sealed with polymethacrylate to prevent medium permeability through the apical foramen. Teeth with any stain (extrinsic or intrinsic) or any other hard tissue developmental anomaly were excluded from the study. A round cavity of 2 mm was prepared on the labial aspect of central incisors and on the buccal aspect of premolars using a straight fissure bur to study the effects of the eight media as mentioned below on the restorative materials. Following cavity preparation, tooth-colored restorative materials, GIC, and composite resin restorative materials were used to fill the cavity to the surface level and polished to remove any surface irregularities. The details of the group and media used in the study are given in Table 1.
| Group | Labeling |
|---|---|
| Groups | |
| Group 1 – Natural teeth | N1 to N8 |
| Group II – Natural teeth with GIC (Type 1) filling | G1 to G8 |
| Group III – Natural teeth with composite filling | C1 to C8 |
| Medium | |
| Commercially available bottled water | M1 |
| Commercial mouthwash | M2 |
| Commercial oil | M3 |
| Chewable tobacco | M4 |
| Filtered smoke | M5 |
| Unfiltered smoke | M6 |
| Coffee | M7 |
| Tea | M8 |
C: Natural teeth with composite filling, G: Natural teeth with GIC filling, N: Natural teeth, M: Medium, GIC: Glass-ionomer cement
As a medium, 5 mL of commercially available bottled water was used. Four grams of coffee, tea powder, and chewable tobacco powder were mixed with 100 mL of bottled water, 5 mL of which was used as the medium for the beverages and chewable tobacco. 5 mL of extra virgin coconut oil was used as the oil. The teeth were placed in a metal container with a lit cigarette or beedi placed on a metal plate to simulate filtered and unfiltered tobacco smoke. Ten 2 mm perforations were made in the plastic lid that sealed the metal container to allow oxygen to enter and burn the cigarette or beedi. Each exposure lasted until two whole cigarettes or beedi were depleted, and this was done 3 times a day. It was ensured that the beedi’s cigarette remained lit throughout the duration of the exposure.
The teeth were preserved in each medium for 24 h before being rinsed with distilled water and cleaned with a brush and paste. The tooth was then placed in a freshly prepared medium (changed every 24 h). This procedure was repeated 6 days in a row for a total of 7 days. On the 7th day of the experiment, all of the teeth were removed from their respective media and cleaned with a new toothbrush to remove any deposited/precipitated medium on the tooth surface. To contrast the natural white color of the tooth surface, the pre-exposure photographs were taken on a black chart background. Post-exposure photographs were taken on a white background to contrast the discoloration or stain deposited on the tooth surface. The amount of discoloration on the crowns of natural teeth, as well as tooth-colored restorative material, GIC, and composite, was compared to a tooth shade guide.
For each of the eight media used in the study, a PowerPoint presentation with eight slides was created, with each slide showing the pre-exposed and post-exposed teeth to one medium. To indicate the intensity of staining on the tooth surface in each medium, a questionnaire was created using a five-point Likert scale with options ranging from mild (1) to severe (5). Four 1st-year undergraduate students were given 30–45 min to view the presentation and complete a questionnaire grading the intensity of staining in the crown and root portions, as well as on the tooth restoration in each medium. The tooth was also provided in case the observer wanted to examine it personally.
Statistical analysis
The responses of the observers were entered into a Microsoft Excel sheet, and the data were analyzed using the Statistical Package for the Social Sciences software. The statistical analyses, two-way analysis of variance (ANOVA) and Tukey post hoc test, were applied to the data obtained. The results are tabulated in Tables 2-4 with graphical representation [Figures 1 and 2].
| Source | Type III Sum of Squares | df | Mean Square | F | Sig. |
|---|---|---|---|---|---|
| Groups and medium | |||||
| Tooth | 10.975 | 2 | 5.488 | 8.826 | 0.000 |
| Medium | 494.095 | 7 | 70.585 | 113.523 | 0.000 |
| Tooth* Medium | 39.431 | 14 | 2.816 | 4.530 | 0.000 |
| Error | 144.250 | 232 | 0.622 | ||
| Total | 1301.000 | 256 | |||
| Portion and medium | |||||
| Portion | 6.413 | 2 | 3.206 | 4.561 | 0.011 |
| Medium | 489.092 | 7 | 69.870 | 99.397 | 0.000 |
| Portion* Medium | 25.160 | 14 | 1.797 | 2.557 | 0.002 |
| Error | 163.083 | 232 | 0.703 | ||
| Total | 1301.000 | 256 |
df: Degrees of freedom, F: F statistic, Sig.: Significance, Statistically significant:P<0.05, *The interaction effect between tooth and medium also between portion and medium.
| Categories | Mean difference | Standard error | Sig. | 95% confidence interval | |
|---|---|---|---|---|---|
| Lower bound | Upper bound | ||||
| Tooth | |||||
| C1 | |||||
| G1 | 0.26 | 0.114 | 0.059 | −0.01 | 0.53 |
| N1 | 0.53* | 0.127 | 0.000 | 0.23 | 0.83 |
| N1 | 0.27 | 0.127 | 0.086 | −0.03 | 0.57 |
| Crown and root portions | |||||
| Crown | |||||
| Restoration | −0.41* | 0.135 | 0.008 | −0.73 | −0.09 |
| Root | −0.20 | 0.121 | 0.233 | −0.48 | 0.09 |
| Root | 0.21 | 0.135 | 0.274 | −0.11 | 0.53 |
Sig.: Significance, Statistically significant:P<0.05, C: Natural teeth with composite filling, G: Natural teeth with GIC filling, N: Natural teeth, *Significant
| Tooth | Portion | M1 | M2 | M3 | M4 | M5 | M6 | M7 | M8 |
|---|---|---|---|---|---|---|---|---|---|
| N 1–8 | Crown | - | Mild color change, blue patches seen along CEJ | - | CEJ shows mild yellow brown | - | Mild change | Yellowish brown | Moderate to severe brown |
| Root | - | - | - | Dark brown | - | Mild change | Dark brown | Dark brown | |
| G1–8 | Crown | - | Mild color change | - | Highly visible yellowish brown | - | Mild change | Moderate to severe mostly around the margin of restoration | Mild to moderate, yellowish brown |
| Root | - | - | - | Dark brown | - | Mild change | Dark brown | Dark brown | |
| Restoration | Mild change | - | - | Moderate to severe changes | No variation but mild change observed by 25% observers | - | Dark yellow to brown (buccal aspect) | ||
| C1–8 | Crown | - | Moderate color change, blue patches seen | - | Highly visible yellowish brown | - | Mild change | Moderate to severe mostly around the margin of restoration. cemento-enamel junction appeared even darker | Moderate to severe, darker than yellowish brown, CEJ darker |
| Root | - | - | - | Dark brown | - | Mild change | Dark brown | Dark brown | |
| Restoration | Mild change | Blue patches surrounding the restoration | - | Moderate to severe changes | No variation but mild change observed by 25% observers | - | Dark yellow to brown (buccal aspect) |
M: Medium, N: Group with natural teeth, G: Natural teeth with GIC (Type 1) filling, C: Natural teeth with composite filling, CEJ: Cemento-enamel junction, GIC: Glass-ionomer cement
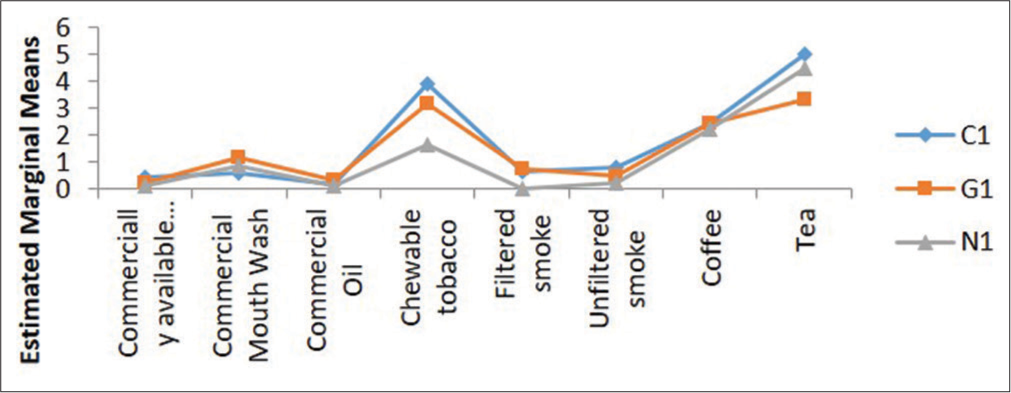
- Estimated marginal means of intensity between groups and medium. C: Natural teeth with composite filling, G: Natural teeth with GIC filling, N: Natural teeth, GIC: Glass-ionomer cement
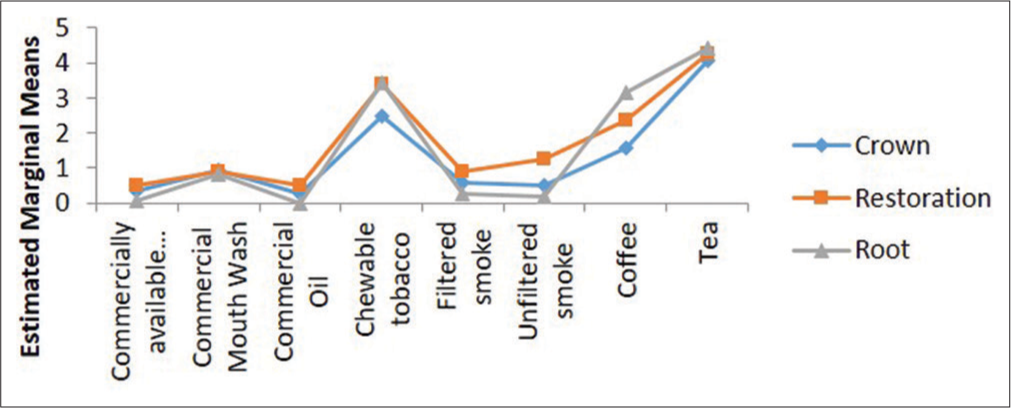
- Estimated marginal means of intensity between portion and medium.
RESULTS
The two-way ANOVA was used to test the significance of the difference in intensity between the three groups and media when comparing tooth types and media. As shown in Table 2, P-value for the tooth, medium, and tooth and medium was 0.000 and significant (Statistically significant – P < 0.05). The two-way ANOVA was used to test the significance of the difference between the portion and the medium. The study’s sections were as follows: Group 1: Crown, Group 2: Restoration, and Group 3: Root. Table 2 shows that P-value was found to be statistically significant in the various portions, media considered, and interaction of portion and medium with P-values of 0.011, 0.000, and 0.002, respectively (Statistically significant - P < 0.05).
Following ANOVA comparing tooth types and media, using the Tukey post hoc test, it was discovered that there is no statistically significant difference in intensity between groups C1 and G1 (P = 0.059), but there is a significant statistical difference (Statistically significant - P < 0.05) in intensity between groups C1, G1, and N1 with P = 0.000, as shown in Table 3. Following ANOVA between the portion and the medium, a Tukey post hoc test was used to determine the effects of iterations in the interaction levels. As shown in Table 3, there is a statistically significant difference (Statistically significant – P < 0.05) in intensity between the portion taken by the crown and restoration (P = 0.008) and no statistically significant difference in intensity between the crown and root (P = 0.233). Figures 3a-c depict the estimated marginal means of intensity between groups and medium, portion, and medium, respectively.
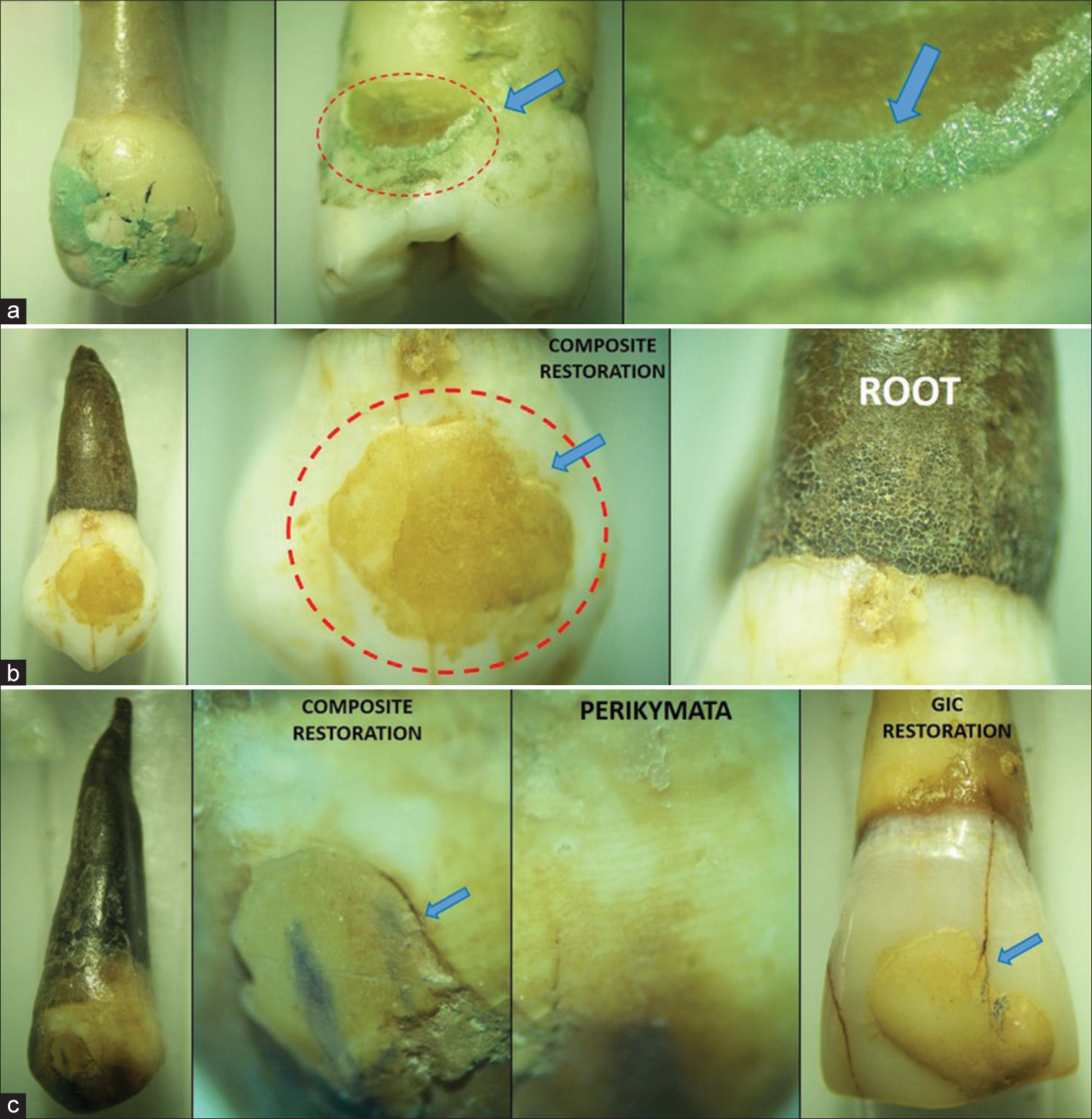
- Staining observed under stereozoom microscope: (a) Commercial mouthwash (M2), Red dashed circle - Cemento-Enamel Junction, blue arrow - higher magnification of Cemento-Enamel Junction. (b) Chewable Tobacco (M4), Red dashed circle - Composite filling taking up stain, blue arrow - junction between tooth and restoration and (c) Coffee (M7), blue arrow - area of staining between restoration and tooth.
Table 4 presents positive and negative findings based on observations made by the primary investigator and blind observers on teeth preserved in eight media. Figure 3 depicts the typical findings for all media as seen through a stereo zoom microscope.
DISCUSSION
The dental tissue enamel is the hard mineralized surface of teeth, with approximately 96% mineralization. The fact that the natural tooth, GIC, and composite restored teeth did not become stained by water demonstrates that the translucency of the enamel was not affected by the constituents of water. If the fluoride or iron content was higher, there would be more pigmentation over the porous enamel. Because the cementum and the restorative materials have the property of water absorption, they absorb water along with its constituents and deposit them in their resin matrix, resulting in a slight variation from their original color [Figure 3].[5]
The two ingredients in mouthwash that cause tooth discoloration are cetyl pyridinium chloride and stannous fluoride. These components adhere to the tooth enamel and deposit over it, resulting in a bluish-black tinge on the surface. A deep blue stain indicates that the mouthwash contains mint flavor with a higher concentration of blue dye. These staining ingredients precipitate stains on teeth when they react with the dietary staining ingredients of beverages.
As a result, patients are advised not to consume a lot of beverages while receiving treatment for certain gum diseases with mouthwashes. The cementum and the restorative materials absorb the liquid, and the components deposit in their resin matrix, causing discoloration.[6]
The teeth and restorations used in this study did not have any stains on the surface of the enamel, cementum, or restoration. This could be due to the fact that the duration of exposure was insufficient to cause any change on the tooth surface.[7,8]
On the crown and root surface, all groups had noticeable staining. This was also observed in other tooth studies. Tobacco stain deposition was more severe, particularly to the cementum, demonstrating that any type of gingival recession can allow tobacco stain to deposit and permeate through the cementum layer.[9]
Although the staining agent’s nicotine and tar in cigarettes are colorless, when they come into contact with atmospheric oxygen, they produce a yellow to brown tinge. This is why chronic smokers who have been smoking for a long time develop a tan on their tooth surface. The tar pigment penetrates deep into the enamel of a restored tooth, penetrating dentin and depositing over the restorations as well. The present study, on the other hand, did not yield positive results. This could be because the teeth were exposed to cigarette smoke for a shorter period of time. A longer time exposure would have resulted in more accurate observations.[4]
Except for the composition, unfiltered smoke – beedi is similar to filtered smoke. However, the nicotine and tar content is higher in this case. The mechanism of discoloration caused by unfiltered smoke is the same as that of filtered smoke. The present study yielded no positive results. This could be due to the insufficient time span of 7 days during which the teeth were exposed to cigarette smoke. A longer time exposure would have resulted in more accurate observations.[10,11]
The roots of the teeth preserved in this medium showed a dark brown discoloration from the cervical to the apical portion as the layer of cementum surrounding the tooth, which is not only thin but also has mineralization similar to that of bone at around 65%. The caffeine and tannins in coffee seep through the pores on the cementum as well as the enamel, causing discoloration. These staining pigments also affect restorations due to their hydrophilicity, which absorbs water and fluids, and their accumulation over time causes discoloration. According to the findings of this study, black tea stains the dental hard tissues, enamel and cementum more than coffee. The dark brown discoloration of the tooth roots from the cervical to the apical portion was observed within minutes of immersing them in the medium.[12-14]
Limitations
Since the present study was conducted with continuous exposure, it was not possible to investigate the role of factors such as saliva and mastication, which provide mechanical cleaning of the tooth surface in the oral cavity.
CONCLUSION
In cases of gingival recession, exposure to common dayto-day fluids can stain the external hard tissue enamel in the crown and cementum exposed in the cervical portion of the root. Chewing tobacco, coffee, and tea were found to have the highest intensity of external stain formation. Even when polished with tea, the staining was observed on GIC and composite restorations, resulting in a generalized light brown color. Unfortunately, because the present study was conducted with continuous exposure, it was not possible to investigate the role of factors such as saliva and mastication, which provide mechanical cleaning of the tooth surface in the oral cavity. Despite the limitations stated above, teeth and dental restorations exposed to different mediums for a short period of time showed significant staining on the enamel and root surface, as well as the margins of dental restorations.
Acknowledgement
The authors acknowledge the support received by the undergraduate student from Indian Council of Medical Research (ICMR), Government of India, New Delhi, under STS program.
Ethical approval
The research/study approved by the Institutional Ethics Committee at Vinayaka Mission’s Sankarachariyar Dental College, number VMSDC/IEC/Approval No. 124, dated 28th March 2019.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- The oral health consequences of chewing areca nut. Addict Biol. 2002;7:115-25.
- [CrossRef] [Google Scholar]
- Color stability of restorative materials in response to Arabic coffee, Turkish coffee and Nescafe. J Contemp Dent Pract. 2013;14:681-90.
- [CrossRef] [Google Scholar]
- Effect of mouth rinses on color stability of resin composites. Eur J Dent. 2008;2:247-53.
- [CrossRef] [Google Scholar]
- Effects of cigarette smoke and tobacco heating aerosol on color stability of dental enamel, dentin, and composite resin restorations. Quintessence Int. 2019;50:156-66.
- [Google Scholar]
- Extrinsic tooth enamel color changes and their relationship with the quality of water consumed. Int J Environ Res Public Health. 2012;9:3530-9.
- [CrossRef] [Google Scholar]
- Effect of different mouthwashes on discoloration of plaque-free tooth surfaces. Am J Dent. 2018;31:211-4.
- [CrossRef] [Google Scholar]
- Oil pulling for maintaining oral hygiene-a review. J Tradit Complement Med. 2017;7:106-9.
- [CrossRef] [Google Scholar]
- Effects of coconut and olive oil on tooth and restoration-in vitro study-myth(oil)ogy? J Acad Dent Educ. 2019;4:22-6.
- [CrossRef] [Google Scholar]
- Effects of cigarette smoking on color stability of dental resin composites. Am J Dent. 2017;30:316-22.
- [Google Scholar]
- Oral health consequences of smokeless tobacco use. Indian J Med Res. 2018;148:35-40.
- [CrossRef] [Google Scholar]
- Effect of various teas on color stability of resin composites. Am J Dent. 2017;30:323-8.
- [Google Scholar]
- Influence of different staining beverages on color stability, surface roughness and microhardness of silorane and methacrylate-based composite resins. J Contemp Dent Pract. 2014;15:319-25.
- [CrossRef] [Google Scholar]




