
Translate this page into:
Don’t Believe What You See in Mouth, Listen To Condyles-A Systemic Review
-
Received: ,
Accepted: ,
This article was originally published by Informatics Publishing and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Centric relation, static and dynamic occlusion are less talked about than its actual importance in dentistry. Their relevance to different disciplines of odontology (general dentistry, conservative dentistry, orthodontics, prosthodontics, dental technicians) has been well documented. Numerous articles in scientific literature regarding the importance and necessity of interdisciplinary teamwork in dentistry to correct problems associated with occlusion has been documented. The centric occlusion and centric relation (CO CR) discrepancy is multifactorial with a degree of psychogenic influence varying throughout an individual’s life with phases of symptoms affecting the quality of life. The current review highlights role of various disciplines in rectifying problems relating to discrepancy in centric occlusion and centric relation.1
1. Introduction
At every level of general practice, a dentist routinely faces problems of sore teeth, excessive wear, loose teeth, Tempeoro-mandibular Joint (TMJ) disorders and oro-facial pain. A dentist who does not have a working knowledge of occlusal principles must resort to guesswork and time-wasting trial and error attempts to solve problems2.3,4.
Gnathologists and restorative dentists have suggested us ing centric relation to pro vide a stable and reproducible posi tion to reconstruct the dentition In recent years, an increased number of dentists desiring to achieve a treatment result wherein the upward and forward or a seated position of the condyle is maintained when the patient closes the mandible to the Intercuspal Position (ICP). Most dentists who look carefully at this joint-to-dentition relationship would agree that the larger the discrepancy between the seated condyle and tooth intercuspation pretreatment, the more difficult it is to achieve the desired result4,5.
2. Why Centric Relation?
Experience with balanced occlusion has taught that unless the maximum intercusping of the teeth is coincident with centric relation of the mandible in the terminal hinge closure, restorations will not work in the mouth as they did on the articulator6,7.
In India concept of checking for interferences in balancing and excursive movements in all patients is lacking resulting in faulty prosthesis and restorations which ultimately affects TMJ and the life of restoration.
Okeson said of centric rela tion that the “most orthopedically stable joint position is when the condyles are in their most superior anterior position in the articular fossa, resting against the posterior slopes of the articular eminences, with the articular discs properly in terposed7.
3. Need for to Rectify CO-CR Discrepancy
Need for rectifying CO-CR discrepancy was highlighted by Ronald H. Roth in his articles on functional occlusion. According to roth need for stability after orthodontic cases partially relied upon functional occlusion5,8,9.
It was then considered necessary to de-programme every case using splint therapy. The dental casts in centric relation on a semi adjustable articulator aided in the diagnosis of the malocclusion. This revealed a malocclusion that is more severe than that seen with teeth in maxi mum intercuspation5,8,9.
Teeth with initial occlusal discrepancies(Figure 1) have significant deeper initial probing depths, worse prognoses, and worse mobility10.
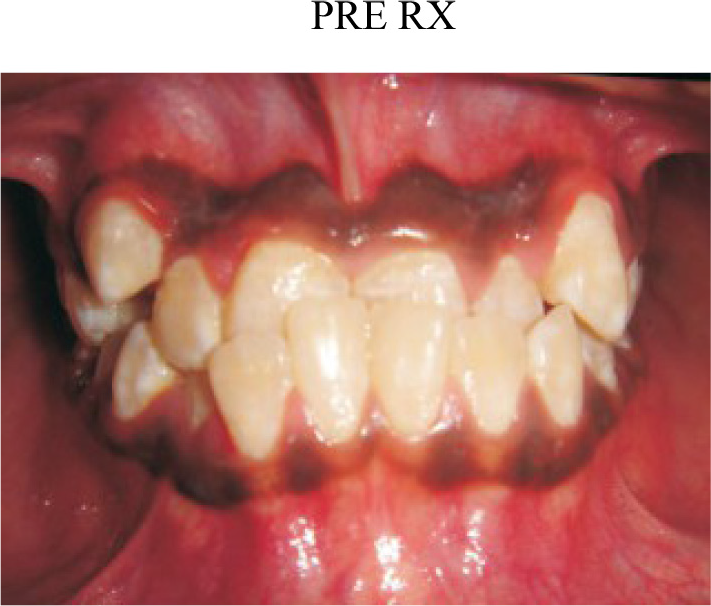
- Teeth with inital occlusal discrepancies.
By increasing the ver tical dimension and separating the posterior teeth, the occlusal interfer ences to centric occlusion are re moved. In the presence of signs and symptoms of temporomandibular dysfunction, a full arch appliance is indicated to limit loading on the joint. These approaches attempt to allow the muscles to relax and allow the condyles to seat more superiorly and anteriorly to reveal the true dis crepancy between the mandibular position in centric occlusion and maximum intercuspation (Figure 3). After finishing it was advocated to use gnatho- positioners to settle in centric11,12,13.
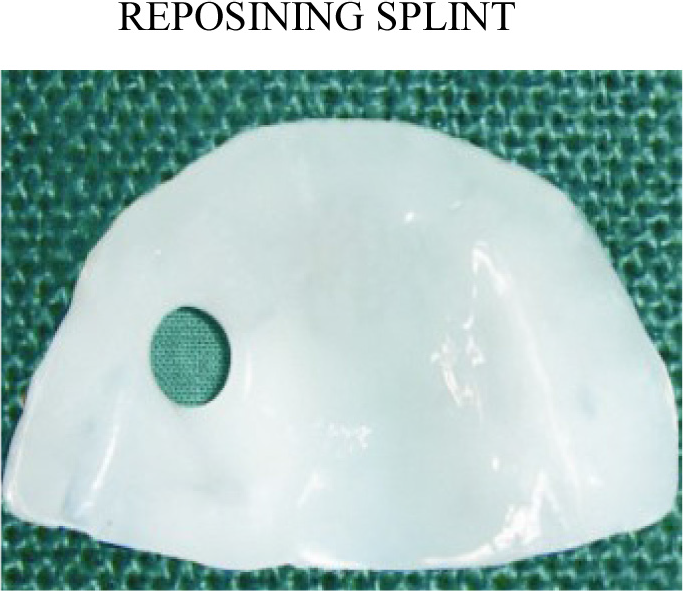
- Oral splint Appliance.
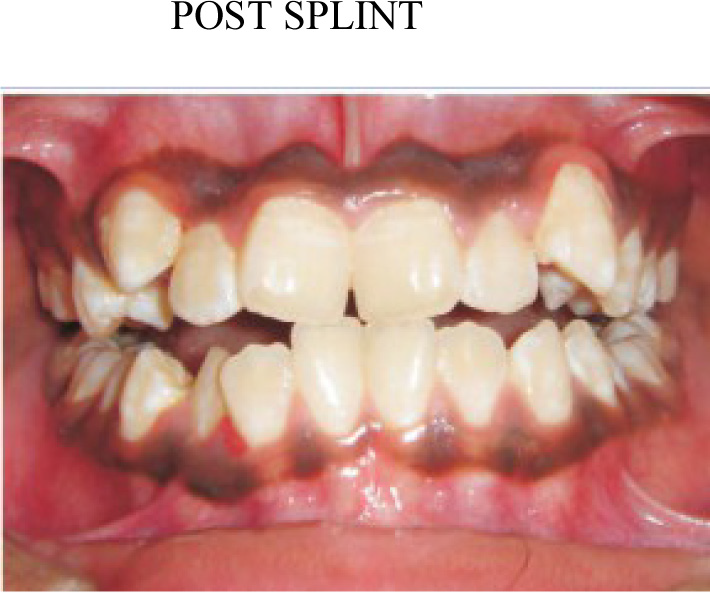
- True malocclusion with condyles seated in fossa.
These removable intra-oral appliances are considered necessary in cases when there is evidence of clinically significant masticatory impairment with documented pain and/or loss of function. Only oral splint (Figure 2) appliance is considered medically necessary for TMD/TMJ therapy14.
The clinical procedures is not a single-day entity, but instead survival on a long-term basis. The clinical longevity of our work is dependent on so many factors and when we have a closer look, all these ultimately depend on the occlusal stability. The restorative dentist must follow the dictates of condylar guidance, and place the cusps properly and construct an anterior guidance that is in harmony with condylar guidance15.
It is important that any case involving an occlusal scheme change start with asymptomatic joints. The joints should be pain-free when firmly loaded with bimanual manipulation, and function without pain from a disk derangement5,14.
Significant number of practitio nershave, for years, advocated mounting (Figure 4) study models in centric relation. These practitioners, along with recent texts, state that it is not an op tional step to be taken on some patients, but a necessary step to be taken on all patients, whether young or adult, because it is not pos sible to accurately predict which cases need to be mounted15.

- Face bow transfer for centric mounting.
4. Rectifying Co-Cr Discrepancy
Presence of occlusal interference is widespread in all population groups, and that there are more people with non-ideal functional occlusal relationships than people with signs and symptoms of functional occlusal disorders. Possible consequences of occlusal interference, such as bruxism and toothwear and relapse of tooth position may also occur sometime after dental treatment16,17.
Splint wear prior to re storative dentistry and orthodontics is indicated when:
The patient exhibits signs and symptoms of TMD;
Difficulty is experienced in recording RCP/ CR;
As a routine, prior to full mouth reconstruc tion orthodontics, and orthognathic surgical pro cedures;
The patient cannot perform reproducible panto-graphic tracings/mandibular movements. Splint wear is continued until:
Signs and symptoms of TMD have been al leviated;
A stable, comfortable, repeatable jaw posi tion has been achieved (as evidenced by stable occlusal contacts on the splint for three months);
The patient can perform reproducible pantographic tracings/mandibular move ments. After checking the patient intraorally, if the patient will not make gliding excursions into protrusive and keep the anterior teeth in contact, you are sure that posterior interference exists. Also if patient cannot make lateral excursions and keep the cuspids together or the patient will not readily allow mandibular manipulation interference exist. Individual tooth positioning needs to be gauged so that they can be moved to achieve an ideal anatomical and functional goal. For this Occlusal equilibration is done. Post treatment cases should not be equilibrated until growth has been completed. The changes with growth are likely to alter the results of equilibration. In orthodontics gnatho-positioners are used to settle occlusion in centric occlusion18–20.
5. Goals of Equilibration11
To establish a positive one-place closure in which centric relation and occlusion are one and the same with equalized occlusal stops for all posterior centric cusps.
To establish proper coupling of anterior teeth and as ideal as possible anterior guidance for posterior disocclusion
To organize the posterior occlusion so as to harmonize ridges and groove direction with mandibular border movements.
To maintain maximum cusp height
To remove a minimum amount of tooth material
To achieve stability of centric relation.
These tech niques predictable and have proven to be faster, easier, less expensive, and more accurate.
6. Conclusion
From the fixed prosthodontist restor ing several quadrants at a time, to the removable prosthodontist fabricating complete dentures, to the oral surgeon positioning the mandible and condyle during orthognathic surgery, the com mon thread is the determination and attainment of a concentric, stable, repeatable condylar posi tion. It is time for the all dental professionals to accept this standard as a treatment goal and to embrace the instrumentation that makes as sessment of this position possible.
References
- Craniomandibular Disorders and Mandibular Reference Position in Orthodontic Treatment. International Journal of Dentistry. 2013;2013 Article ID 890942
- [Google Scholar]
- Response of patients with pain-dysfunction syndrome to mock equilibration. J Am Dent Assoc. 1976;92:755-8.
- [Google Scholar]
- Occlusion, orthodontic treatment, and temperomandibular disorders. A review. J Orofacial Pain. 1995;9:73-90.
- [Google Scholar]
- Occlusion: The gateway to success. Journal of Interdisciplinary dentistry. 2012;2:68-77.
- [Google Scholar]
- Okeson - Management of Temporomandibular Disorders and Occlusion (6th ed). Elsevier Health Sciences; 2008.
- [Google Scholar]
- The use of a deprogramming appliance to obtain centric relation records. Angle Orthod. 1999;69(2):117-24.
- [Google Scholar]
- Nunn The Effect of Occlusal Discrepancies on Periodontitis. I Relationship of Initial Occlusal Discrepancies to Initial Clinical Parameters. Journal of Periodontology. 2001;72:485-494.
- [Google Scholar]
- Comparison of Condylar Position in Hyperdivergent and Hypodivergent Facial Skeletal Types. Angle Orthodontist. 2001;71(4)
- [Google Scholar]
- Hess Restoring the Functional Zone: Correcting Anterior Constriction with Centric Relation-Based Inside Dentistry. . 2007;3(9)
- [Google Scholar]
- Centric relation treatment and articulator mountings in orthodontics. The Angle Orthodontist. 1996;66:153-8.
- [Google Scholar]
- Occlusal interferences and functional disturbances of the masticatory system. Clin Periodontol. 1974;1:12-9.
- [Google Scholar]




