
Translate this page into:
Trauma-induced ectopic eruption: A novel approach – A case report with review of literature
 , Srirengalakshmi Muthuswamy Pandian2, Sumaiyya Saleem1
, Srirengalakshmi Muthuswamy Pandian2, Sumaiyya Saleem1

*Corresponding author: Sushanthika Asokan, Undergraduate Student, Department of Pediatric and Preventive Dentistry, Sathyabama Dental College and Hospital, Chennai, Tamil Nadu, India. sushanthashokan9962@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Ashokan S, Anand S, Kalaivanan D, Muthuswamy Pandian S, Saleem S. Trauma-induced ectopic eruption: A novel approach – A case report with review of literature. J Academy Dent Educ. 2024;10:118-21. doi: 10.25259/JADE_85_2023
Abstract
Guiding the eruption for the development of functionally stable and socially acceptable occlusion in children is crucial on a pediatric dentist’s perspective. Ectopic eruption refers to a condition where a tooth deviates from its normal path of eruption and is not in its usual position Ectopic eruption mostly involve maxillary incisors, accounting for about 5 percent. In primary dentition, luxation injuries are the most prevalent kind of TDI. Permanent incisors are at a higher risk of developing post-traumatic complications because they are closely related to the apices of primary incisors.Usually, fixed appliances are used to treat such ectopic eruption. This case report discusses the successful management of an 8-year old Indian boy who had an unusual ectopic eruption of his maxillary left central incisor by a novel removable appliance approach.
Keywords
Incisor
Tooth
Deciduous
Orthodontic Appliances
Fixed
Tooth Eruption
Ectopic

INTRODUCTION
The natural process by which a tooth enters the alveolar process bone, and the oral epithelium to articulate with its opponent and transition from its developing position to its functioning position is known as dental eruption. When the periodontal ligament begins to form, this process begins.[1] The pathway for new tooth eruption is determined by the root resorption rate rather than the root formation rate. Once the eruption path is established, the tooth moves occlusally.[2] However, local or inherited factors may disrupt the natural eruption of one or more teeth. The precise mechanism is still unknown because of the slow speed of tooth eruption and the difficulties of seeing it.[1]
Most of the teeth eruption challenges develop during the transitional dentition stage, one of which is ectopic eruption. Ectopic eruption refers to a condition where a tooth deviates from its normal path of eruption and is not in its usual position.[3] Early detection and treatment may aid in the prevention of a more complicated malocclusion. Malocclusion decreased arch length, and inadequate space for the succedaneous premolar might arise from the untreated ectopic eruption.[4]
In primary dentition, luxation injuries are the most prevalent kind of traumatic dental injury (TDI).[5] Permanent incisors are at a higher risk of developing post-traumatic complications because they are closely related to the apices of primary incisors. In up to 69% of cases, damage to primary teeth can disrupt the development of permanent teeth varying from minor enamel opacities to more severe conditions such as delayed eruption, root arrest, and permanent tooth non-eruption.[5,6] This case report describes the occurrence and management of ectopic eruption of maxillary permanent central incisor due to trauma to the primary teeth and its successful management using a novel modified removable appliance.
Intrusion of primary teeth can cause succedaneous teeth’s ectopic eruption. This happens when a baby tooth is pushed too far into the gums, causing the permanent tooth to erupt ectopically. Intrusive luxation is responsible for causing 4.4–22% of primary TDI. A significant injury to the predecessor may result in the permanent incisor’s ectopic eruption.[7,8] The permanent germ may have been physically displaced, the premature loss of the primary incisor may not have offered eruption guidance, or both may be to blame for the problem.[8]
CASE REPORT
An 8-year-old Indian boy appeared at our private practice 3 months ago with the chief complaint of an unerupted upper left central incisor. According to reports, the youngster was 4 years old when he suffered an injury to his upper primary incisors (luxation injury on anamnesis of his parents) and was treated for pulp necrosis in another location. Clinical examination revealed Grade 3 mobility in the primary maxillary laterals, with the maxillary left central (21) ectopically erupting in the vestibular sulcus. Further inspection revealed that the growing centrals had adequate space for teeth eruption with the permanent molars in Class I occlusion. It was planned to intervene with a modified removable Hawley’s appliance with a labial bow incorporating hooks and elastics attached to Begg’s bracket bonded to 21 [Figure 1] after informed consent and discussion with parents. To avoid future issues, alignment and extrusion of 21 was planned orthodontically. There was clinically substantial extrusion of 21 and alignment into the arch after 6 weeks of compliant use by the individual [Figure 2].
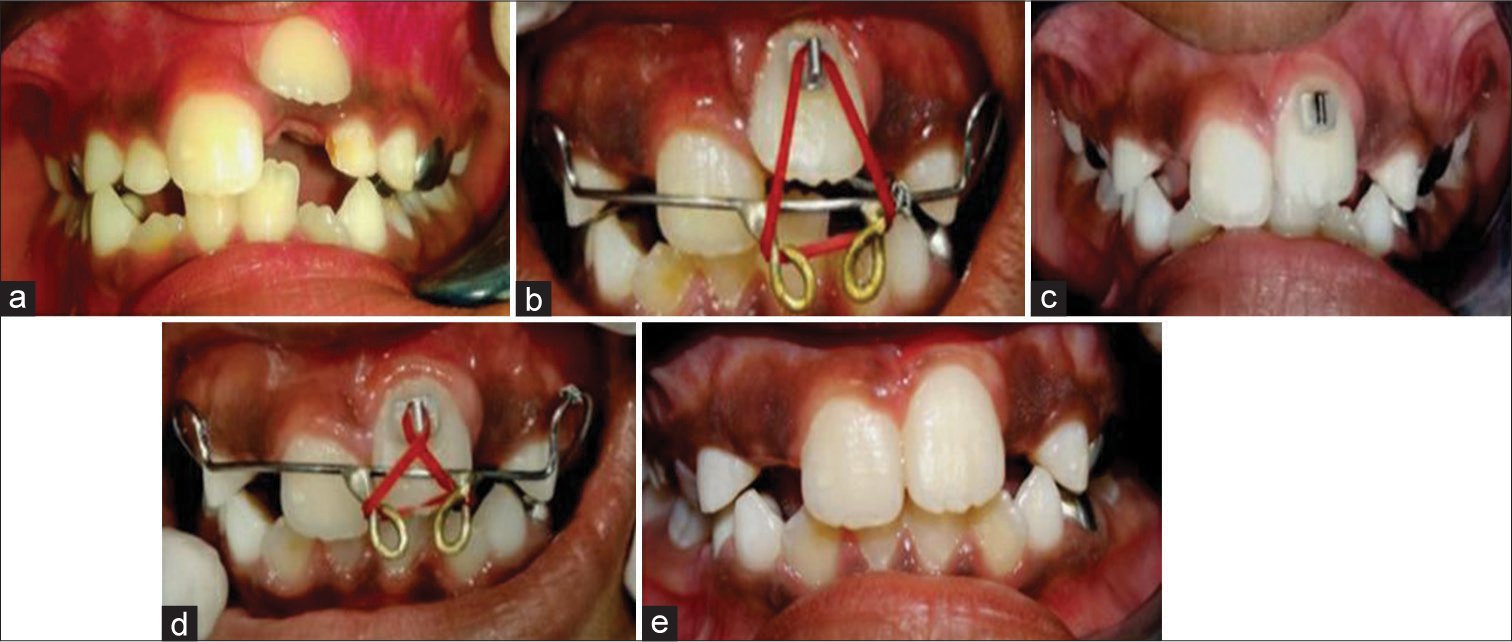
- (a) Ectopic eruption of upper left permanent central incisor 21, (b) Single elastics and active engagement with Begg’s bracket bonded in 21, (c) Review after 2 weeks exhibiting extrusion and eruption of 21, (d) Double elastics engagement for 4 weeks, (e) Post op clinical view after 6 weeks with the tooth 21 aligned in proper position.

- Modified Hawley’s appliance with incorporated loops in labial bow to engage 3/16” elastics.
DISCUSSION
Studies suggest that more than half of all ectopic eruptions occur in the upper and lower permanent central incisors.[9] Ectopic eruption of teeth can happen in various locations, including the palate, condyle, maxillary sinus, orbit, and even through the skin.[10] A number of conditions, including supernumeraries, retained deciduous teeth, major damage to primary teeth, tooth size-arch length disparity, cleft palate, and any congenital developmental problem, can result in the ectopic eruption of permanent teeth. Suspicion of delayed eruption can develop when there is a disrupted eruption sequence or the presence of an unerupted tooth for more than 6 months when compared to the contralateral tooth.[6,11]
Traumatic injuries, particularly luxation injuries, can cause tooth germ displacement or a lack of eruption guidance from prematurely lost primary incisors and thus interrupt eruption.[6] Intrusion of primary teeth in specific can cause succedaneous teeth’s ectopic eruption. This happens when a baby tooth is pushed too far into the gums, causing the permanent tooth to erupt ectopically. Intrusive luxation is responsible for causing 4.4–22% of primary TDI. A significant injury to the predecessor may result in the permanent incisor’s ectopic eruption.[7,8] The permanent germ may have been physically displaced, the premature loss of the primary incisor may not have offered eruption guidance, or both may be to blame for the problem.[8]
Fixed appliances, such as open coil springs and modified fan-shaped appliances, have been employed to regulate ectopic incisor eruption resulting from reported trauma and abnormal eruption trajectory.[9,12] Our novel removable Hawley’s appliance technique could be a viable option for pediatric patients resisting the use of such fixed appliances. In this case, we used orthodontic elastics (3/16”) for 6–12 h/day for 6 weeks and patient was asked to change the elastics for every 2 days. This resulted in the clinical extrusion of the affected upper left central incisor. We also activated the labial bow for 2 weeks, which caused retraction. A previous study revealed that orthodontic therapy for ectopic eruption causes gingival discrepancies.[13] In our case, the use of modified removable appliances produced mild pressures that efficiently achieved clinically acceptable gingival levels.
CONCLUSION
This novel appliance presents a potential solution to the use of fixed appliances in the management of ectopic eruption during the early mixed dentition period.
This approach could also be a judicious choice for the orthodontic extrusion of young permanent incisors following intrusion injuries.
It should be noted that trauma experienced during primary dentition specifically intrusion necessitates careful monitoring as it may result in unforeseen developmental abnormalities of the permanent teeth.
Acknowledgments
We would like to express our sincere gratitude to the Department of Orthodontics, Saveetha Dental College and Hospital for their valuable technical assistance.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflict of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Mechanism and control of tooth eruption: Overview and clinical implications. Orthod Craniofac Res. 2009;12:59-66.
- [CrossRef] [PubMed] [Google Scholar]
- Primary failure of eruption (PFE): A systematic review. Head Face Med. 2018;14:5.
- [CrossRef] [PubMed] [Google Scholar]
- Tooth transposition literature review and a clinical case. Braz J Oral Sci. 2006;5:953-7.
- [Google Scholar]
- Ectopic eruption-A review and case report. Contemp Clin Dent. 2011;2:3-7.
- [CrossRef] [PubMed] [Google Scholar]
- International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: General introduction. Dent Traumatol. 2020;36:309-13.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of traumatic dental injuries to primary teeth on permanent teeth-a clinical follow-up study. Dent Traumatol. 2010;28:1-5.
- [Google Scholar]
- Textbook and color atlas of traumatic injuries to the teeth New Jersey: Wiley-Blackwell; 2007.
- [Google Scholar]
- Intrusion injuries of primary incisors. Part III: Effects on the permanent successors. Quintessence Int. 2000;31:377-84.
- [Google Scholar]
- Ectopic eruption of maxillary central incisor through abnormally thickened labial frenum: An unusual presentation. J Indian Soc Pedod Prev Dent. 2017;35:94-7.
- [CrossRef] [PubMed] [Google Scholar]
- Ectopic eruption of maxillary molar tooth-An unusual cause of recurrent sinusitis. Singapore Med J. 2001;42:801.
- [Google Scholar]
- National clinical guidelines for the management of unerupted maxillary incisors in children. Br Dent J. 2018;224:779-85.
- [CrossRef] [PubMed] [Google Scholar]
- Unusual ectopic eruption of a permanent central incisor following an intrusion injury to the primary tooth. J Can Dent Assoc. 2008;74:723.
- [Google Scholar]
- A case of an unerupted maxillary central incisor for indirect trauma localized horizontally on the anterior nasal spine. J Clin Pediatr Dent. 2005;29:201-3.
- [CrossRef] [PubMed] [Google Scholar]




