
Translate this page into:
Taurodontism in primary molars: A case report

*Corresponding author: Akanksha Juneja, Professor, Department of Pediatric and Preventive Dentistry, Faculty of Dentistry, Jamia Millia Islamia, New Delhi, Delhi, India. ajuneja@jmi.ac.in
-
Received: ,
Accepted: ,
How to cite this article: Chaudhary A, Sultan A, Juneja A. Taurodontism in primary molars: A case report. J Academy Dent Educ. 2024;10:43-6. doi:10.25259/JADE_24_2023
Abstract
Taurodontism is a development disorder involving large pulp chambers with the furcal areas located closer to the root apex. The crowns of teeth associated with taurodontism appear normal and its distinguishing features are present below the cementoenamel junction. This makes the radiographic evaluation crucial for its diagnosis. Taurodontism is more commonly found in permanent teeth than in deciduous teeth. Taurodontism occurs mostly as a lone anomaly. Still, it is associated with certain syndromes including Down’s syndrome (Trisomy 21), Klinefelter’s syndrome, and a few medical conditions such as hypophosphatasia. From the perspective of endodontics, taurodontism demands greater efforts for root canal therapies than for a tooth with a normal pulp chamber. The reason is larger pulp chambers that pose obturation errors in the tooth and increase failure percentage. This paper discusses taurodontism associated with primary molars in a 4-year-old dental patient.
Keywords
Dental anomaly
Enlarged pulp chambers
Shifman and Chanannel criteria
Taurodont teeth
Taurodontism

INTRODUCTION
The word taurodontism involves the incorporation of two terms “tauros,” representing “bull” in Latin, and “odus” in Greek refers to “tooth.” It is a developmental disorder involving large pulp chambers with the furcal areas located closer to the root apex.[1] Taurodontism was a typical finding observed in Neanderthal man, but this anomaly was not so commonly seen in Modern man.[2] However, an increasing number of recent case reports in the dental literature reveal that taurodontism is no longer a rare anomaly in today’s man. It has been reported both in permanent dentition as well as deciduous dentition.[3] More frequently involved teeth are of permanent dentition than deciduous dentition. Taurodontism is usually seen as a lone entity but may also be present in conjunction with a few syndromes.[1] There is uncertainty about the factors responsible for taurodontism. A few researchers recommend this as a consequence of Hertwig’s sheath’s inability to invaginate at an appropriate horizontal point.[3] Taurodontism leads to certain changes in normal tooth anatomy. The enlarged pulp chambers and the apical placement of the furcation region give teeth a “bull” like appearance. In a few instances, the radicular furcation is only a few millimeters far from the root apex. The crowns of taurodont teeth appear normal and their distinguishing features are present below the cementoenamel junction (CEJ). This makes the radiographic evaluation crucial for its diagnosis. The diagnostic criteria for taurodontism involve the presence of a larger than normal pulp chamber, downwardly displaced pulpal floor, with missing constriction at the CEJ.[4,5]
In this article, we discuss a 4-year-old male patient without any associated syndrome or medical condition presenting with taurodontism in primary molars in maxillary and mandibular arches.
CASE REPORT
A 4-year-old male child visited the outpatient department (OPD) with pain in the left mandibular molars. The pain was mild and intermittent but aggravated on eating and subsided on its own. The patient did not complain of any other pathology or abnormal findings related to medical history. The child was born preterm (8 months) with normal delivery, and the mother did not report any pre- or post-natal defects; or any familial history of dental anomaly. On clinical evaluation, the crowns of primary molars were normal-shaped with the presence of dental caries with 74, 75, 84, and 85. The carious tooth was tender on percussion and showed no signs of gingival inflammation, observable swelling, or sinus involvement. Since 75 had a deep carious lesion, intraoral periapical radiograph (IOPA) was advised. The radiographic evaluation indicated the characteristic signs of taurodontism with caries approaching the pulp of the teeth 74 and 75. Radiologically, crowns of molars appeared to be larger at the cost of roots. The pulp chambers and the bifurcation of roots were located much apically below the CEJ. The constriction at the level of CEJ was insignificant [Figure 1].

- The intraoral radiograph shows deep occlusal caries (75) enlarged pulp chambers and apically shifted bifurcation (74, 75).
Based on radiographic examination, an orthopantomogram (OPG) was advised to rule out the presence of Taurodontism in other teeth. A panoramic radiograph showed multiple molars with taurodontism. 55, 65, 74, 75, 84, and 85 had enlarged pulp chambers with short roots. No other anomalies were noticed on OPG [Figure 2].
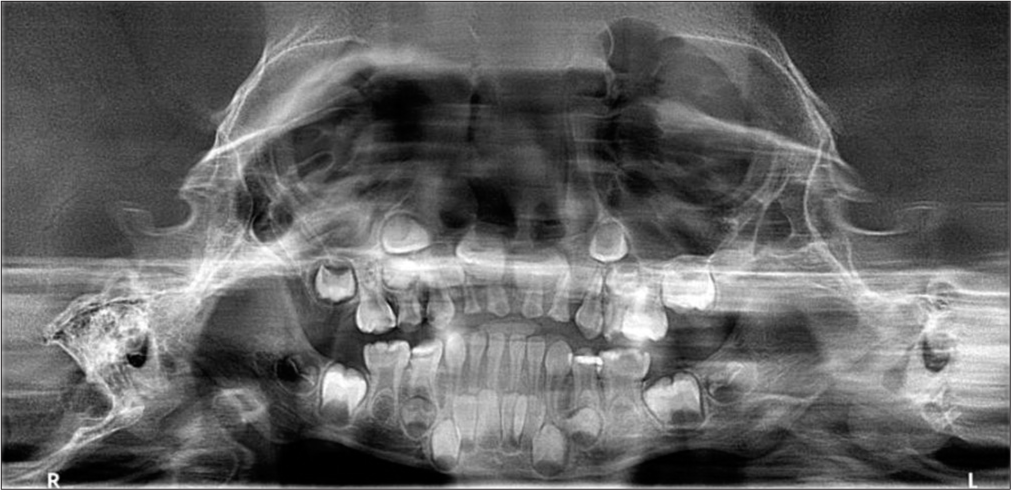
- Orthopantomagram revealed an enlarged pulp chamber in all primary molars.
In the OPG, 64 and 65 teeth were unclear, so an IOPA of this region was taken. The characteristics and findings of taurodontism in 64 and 65 were not clear as the involvement of the roots of the molars was still inconspicuous [Figure 3].

- An intraoral periapical radiograph of the 6th quadrant.
For the diagnosis of taurodontism, we applied Shifman and Chanannel 1978 principle.[5] For this, we evaluated the location of points A and B in the pulp chamber outline: Point A as the lowest spot occlusally and Point B as the highest juncture apically. Distances were measured as follows:
The stretch between point A and B/the length from point A to the tip of the longest root (this value should preferably be ≥ 0.2)
Measurements from point B to the cementoenamel junction should be ≥2.5 mm
-
Categories or subtypes:
– Hypotaurodontism: 20–20.9%
– Mesotaurodontism: 30–39.9%
– Hypertaurodontism: 40–75%
In this case, the a/b = The stretch between point A and B/Length from A to Root tip = 0.53 for 54, 0.54 for 55, 0.50 for 74, 0.37 for 75 and 85, and 0.35 for 84 [Figure 4].
![Tracing of the intraoral periapical radiograph showing 74, 75, 84, 85, 54 and 55 confirming the taurodontic tooth according to Shifman and Chanannel criteria.[5]](/content/121/2024/10/1/img/JADE-10-043-g004.png)
- Tracing of the intraoral periapical radiograph showing 74, 75, 84, 85, 54 and 55 confirming the taurodontic tooth according to Shifman and Chanannel criteria.[5]
From the radiographic findings, six molars showed taurodontism including three hypertaurodonts (#54, #55, and #74), and three mesotaurodonts (#75, #84, and #85). The patient’s parents were counseled and briefed about the clinical situation. Based on clinical and radiographic findings, an indirect pulp capping was done in 75, restorations were done in 74, 84, and 85. The patient was recalled after 4 weeks for a review check-up.
DISCUSSION
According to Witkop, a taurodont tooth refers to one with enlarged pulp chambers with the apically displaced root bifurcation or trifurcation, resulting in an elongated apicoocclusal width of the pulp cavity and lack of constriction at the cervical area of the tooth.[6] Based on Feichtinger and Rossiwal’s findings, the measurements between the cervical area of a crown to the furcation point in roots must be more than the cervicoocclusal stretch for a tooth to be classified as taurodont.[7]
Taurodontism is also seen in conjunction with several well-known syndromes such as Down’s syndrome, Klinefelter’s syndrome, and a few medical conditions such as hypophosphatasia. Very rarely, the taurodontic trait was also found and reported with some other diseases such as Ameloonchyo-hypohidrotic syndrome, hereditary ectodermal dysplasia, or Hypohidrotic ectodermal dysplasia related to X-chromosome. This feature is also seen in systemic aberrations such as microcephalic dwarfism and specific oral developmental abnormalities such as agenesis or fusions, amelogenesis imperfecta, and dermatologic disturbances.[8]
With increasing time, researchers have reported newer concepts related to the pathogenesis of taurodontism. It includes a unique pattern of development, a delay in pulpal chamber calcification, absence or lack of odontoblasts, and a variation in the arrangement of epithelial cells present in the cervical loop of the enamel organ hertwig’s epithelial root sheath (HERS) resulting in a delay or inability to merge of the horizontal flaps of the epithelial diaphragm.[1]
As suggested by Mangion in his article,[9] the possible etiological causes of taurodontism could be either of these. “A primitive pattern;” “A Mendelian recessive trait;” “An atavistic characteristic;” “A mutation;” and “A special or retrograde feature.”
Based on published data, the occurrence of taurodontism in permanent dentition ranges from 2.5% to 3.2%, and it occurs in 0.54% of primary teeth.[1] Although this condition is more prevalent in females (52%) than males (48%), the dental literature does not highlight statistical significance. Since taurodontism is linked to the X-chromosome, the high prevalence in females is relevant.[10] According to some genetic studies done in individuals with extra X-chromosomes, such as 47, XXY boys (Klinefelter’s syndrome), the X-chromosome includes a gene responsible for the development of a taurodont tooth.[1] In addition, taurodont teeth are diagnosed frequently in the maxillary arches compared to the mandibular arches, and maxillary molars (57%) are the most frequently involved teeth compared to mandibular molars (43%). The frequently observed taurodontism type is hypotaurodontism, having a prevalence of 94%.[10]
It can present in any combination of teeth or regions in the jaws, singly or bilateral.[1] In our patient, taurodontism was present in the primary dentition and radiographically evident in the 5th, 7th, and 8th quadrants, while the involvement of the 6th quadrant was unclear. Another intraoral periapical radiograph for the latter revealed taurodontism, but the involvement of the roots of the molars was still inconspicuous [Figure 4].
Clinical implications
Many dental treatments are adversely affected by taurodontism, particularly endodontics therapy, as it involves difficulties during root canal negotiation, biomechanical preparation, and obturation.[11] The shapes and sizes of pulp chambers in taurodont teeth vary significantly. These teeth may present with complex root canal systems involving various obliterations, low canal openings, and extraradicular canals. Considering the huge frustrations faced during root canal therapies in teeth involving taurodont, the attention received by the topic is minimal. Certain endodontic therapies repeatedly fail due to the lack of clinical judgment skills for handling such cases. The use of ultrasonic irrigation, a modified clinical method, and careful examination of the orifices, particularly when magnified, are of utmost importance.[9] There are chances of taurodont teeth having unusual patterns of root canals, making it tougher for dentists to perform endodontic therapies.[10] Due to large pulp chambers, proper obturation of the root canals in taurodont teeth becomes difficult. Therefore, dental experts have recommended an altered way of obturation, which involves lateral compaction at the root apex alongside vertical compaction of the abnormally elongated pulpal cavities.[12] Considering our case if there would have been pulpal involvement of caries, then adequate precautionary measures would have to be taken.
Although cases of taurodontism have been reported in primary dentition in the past, the number is very low. More and more cases need to be available in the literature so that variations and alterations can be observed and accordingly, comprehensive treatment can be provided. Furthermore, reporting of cases helps in the estimation of the overall incidence and prevalence of under-reported conditions like taurodontism.
CONCLUSION
Taurodontism being a rare anomaly, does not reduce its clinical significance. Every dental practitioner should be aware of this dental anomaly and have comprehensive insight regarding the identification and treatment to prevent pain sequelae or endodontic failures, as adequate identification plays a key role in determining the treatment plan and prognosis of taurodontic teeth.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Taurodontism in deciduous molars. BMJ Case Rep. 2013;2013:bcr2013010079.
- [CrossRef] [PubMed] [Google Scholar]
- Taurodontism in deciduous molars-a case report. J Indian Soc Pedod Prev Dent. 2004;22:193-6.
- [Google Scholar]
- Taurodontism an endodontic enigma: A case report. Indo Eur J Dent Ther Res. 2017;5:377-9.
- [Google Scholar]
- Prevalence of taurodontism found in radiographic dental examination of 1,200 young adult Israeli patients. Community Dent Oral Epidemiol. 1978;6:200-3.
- [CrossRef] [PubMed] [Google Scholar]
- Manifestations of genetic diseases in the human pulp. Oral Surg Oral Med Oral Pathol. 1971;32:278-316.
- [CrossRef] [PubMed] [Google Scholar]
- Taurodontism in human sex chromosome aneuploidy. Arch Oral Biol. 1977;22:327-9.
- [CrossRef] [PubMed] [Google Scholar]
- Endodontic management of taurodontic teeth. Indian J Dent Res. 2005;16:177-81.
- [CrossRef] [PubMed] [Google Scholar]
- Taurodontism--prevalence, extent, and clinical challenge in Ashkelon, Israel--a retrospective study. Appl Sci. 2022;12:1062.
- [CrossRef] [Google Scholar]
- Taurodontism: An endodontic challenge. Report of a case. J Endod. 2003;29:353-5.
- [CrossRef] [PubMed] [Google Scholar]
- "Taurodontism" an endodontic challenge: A case report. J Oral Sci. 2009;51:471-4.
- [CrossRef] [PubMed] [Google Scholar]




