
Translate this page into:
Rapid Maxillary Expansion and Appliance
*Address for correspondence:
This article was originally published by Informatics Publishing and was migrated to Scientific Scholar after the change of Publisher.
Abstract
The purpose of this article is to know more about the rapid maxillary expander. It produces significant changes in the maxillary arch. RME has fundamental effect on the dentofacial structures which results in major change occurring in the basal structures of the maxilla. The concept of maxillary expansion has also been extended to the nasal cavity. Early orthodontic treatment with RME is able to reduce the symptoms of obstructive sleep apnea syndrome. This technique is more suited for younger patients and faster duration of action.
Keywords
Obstructive Sleep Apnea Syndrome
Rapid Maxillary Expander

1. Introduction
RME is otherwise known as Rapid palatal expander or split palate. RME produce skeletal type of expansion. It consists of enlargement of dental arch and widening of the palate. This concept was widely supported by ENT surgeons. RME is more useful in mixed dentition. It places an important role in the orthopaedic therapy. Orthopaedic expansion is the procedure by applying a lateral force against the posterior maxillary dentition producing a separation of midpalatal suture and produces increase in the transverse width of maxillary basal bone1,2.
2. Effect of the Rapid Maxillary Expansion
2.1 Effect on Maxillary Teeth
In anterior teeth, RME opens the midpalatal suture which creates midline spacing between two maxillary central teeth, Bodily displacement of tooth along its long occlusal direction of molars in the posterior teeth3,4.
2.2 Effect on Mandible
Decreases the overbite and increases the facial height of the mandible because of the extrusion and buccal tipping of the maxillary molars4.
2.3 Effect of RME in Nasal Cavity
Increase the intranasal space due to separation of the outer walls during activation of RME. Patients with narrow maxillary arch along with malocclusion can lead the OSAS. So RME is more affective in patient with OSAS2,4.
2.4 Effect on Alveolar Bone
During activation of RME because of compression of periodontal ligament the alveolar bones bends buccally5.
3. Indication
4. Contra Indication
Medically compromised patient.
Patient with poor co-operation.
Not accepted for deciduous dentition.
Handicapped patient.
Before completion of midpalatal suture RME is not accepted.
Patients with steep mandibular plane angle.
5. Types of Appliance Used for RME
Removable
-
Fixed – Divided into two types
- A Banded
- B Bonded
5.1 Banded RME
Tooth borne and tissue borne.
Tooth borne.
5.1.1 Tooth Borne and Tissue Borne
Derichsweiler type.
Hass tyre.
5.2.2 Tooth Borne
Isaacson type.
Hyrax type.
5.2 Bonded Type RME
Cast cap splints.
Acrylic splints1.
6. Fixed Appliance
6.1 Derichsweiler Type
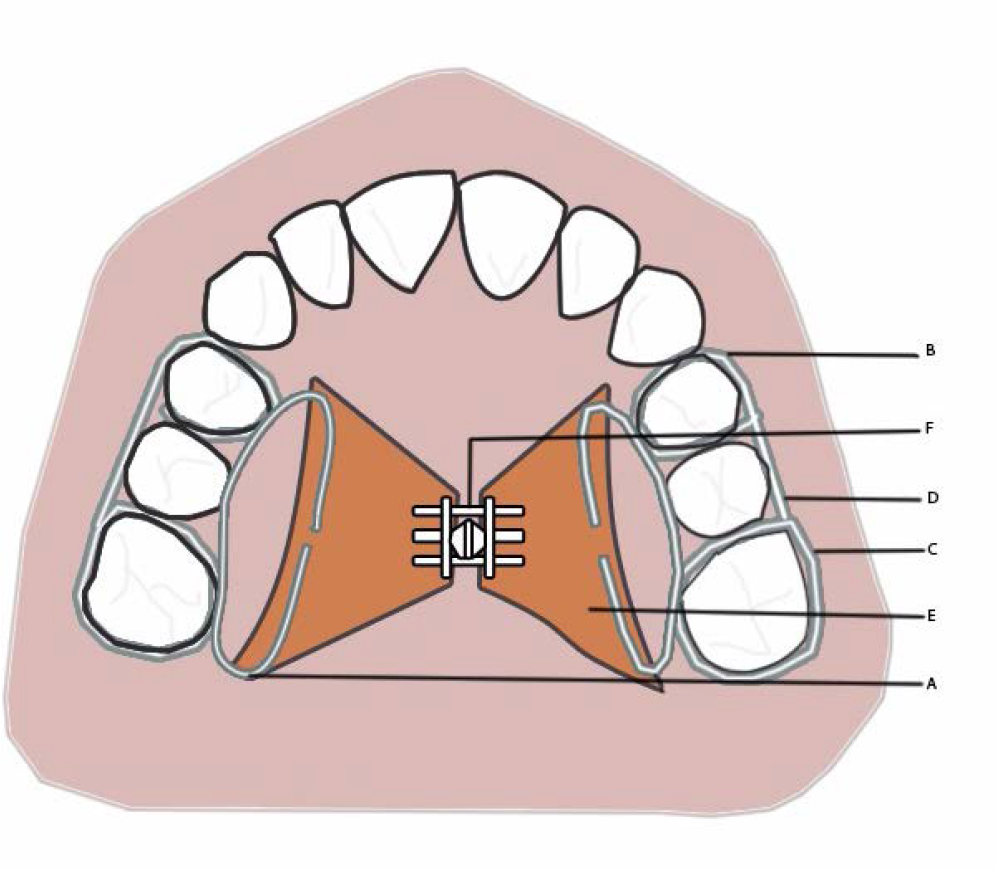
This appliance is tooth tissue and tooth borne type of appliance and also banded fixed appliance. The molar and premolar are banded. Wires are tagged and soldered onto the palatal aspect of the band. Those wires tags are inserted into a splitpalatal acrylic plate, incorporating a screw at its centre5,8,9. [Figure 1]

- Derichsweiler type of expansion appliance
- a. Wires tags.
- b. Premolar bands.
- c. Molar bands.
- d. Expansion screw.
- e. Acrylic plate.
6.2 Hass Type
The Hass type expander is a tooth and tissue borne style of appliance that consists of bands. The first molar and premolar are banded with a midline screw, incorporated into two acrylic plates which connect with the mucosa of the palate. Supported wires are extended to the anterior of the molar along with the posterior molar in order to get rigidity. Acrylic plates are used to reduce the tipping of the posterior molars. Inflammation of the palatal tissue due to contact of appliance with the palate.1,5,9 [Figure 2]
- Hass type of expansion appliance
- a. Lingual support wire.
- b. Premolar bands.
- c. Molar bands.
- d. Buccal support wire.
- e. Acrylic plate.
- f. Expansion screw.
6.3 Hyrax Type
The Hyrax tyre of expander is a fixed tooth borne appliances that consist of bands. The bands are connected to the first molar and premolar with Hyrax screw incorporated into the metal framework. Acrylic component are not used in the fabrication of the Hyrax appliance. Hyrax appliance is more flexible when compared to the Derichsweiler and Hass type expander1,5,9. [Figure 3]
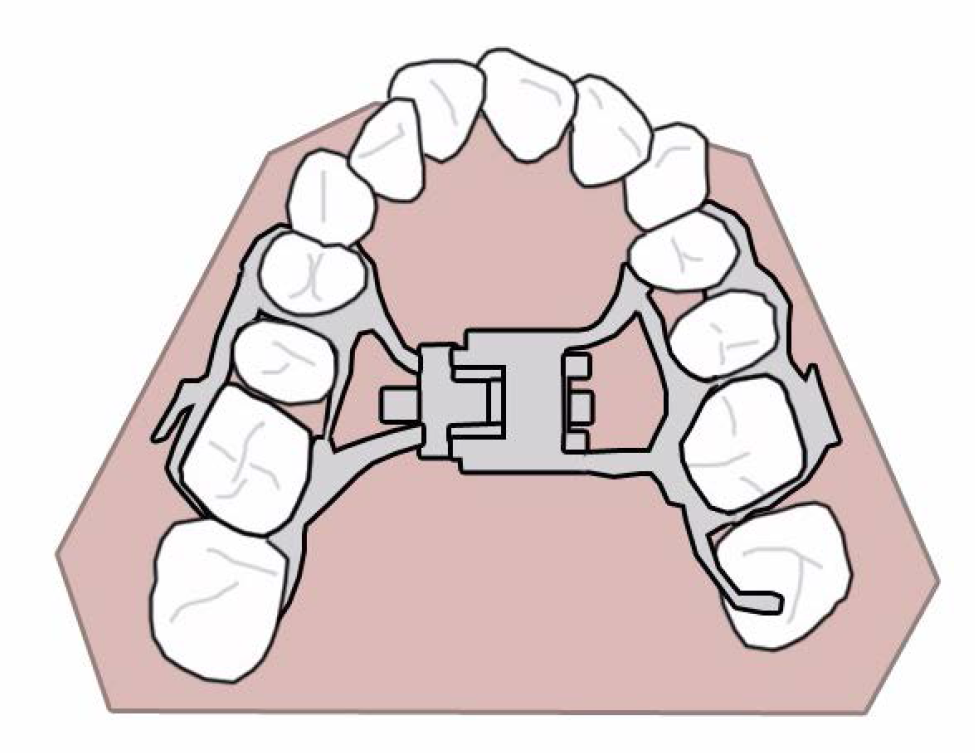
- Hyrax type of expansion appliance.
6.4 Isaacson Type
Isaacson type of expander is a tooth borne appliance instead of acrylic component metal frame work is used. MINNE expander (developed at the University of Minnesota, dental school) is a type of spring loaded screw in Isaacson type of expander. The first molar and premolar are soldered and banded into the lingual and buccal aspect using metal framework. This type of expander contains coil spring which compresses the spring having nut. The Isaacson expander is activated by closing the nut which compresses the spring7–9. [Figure 4]
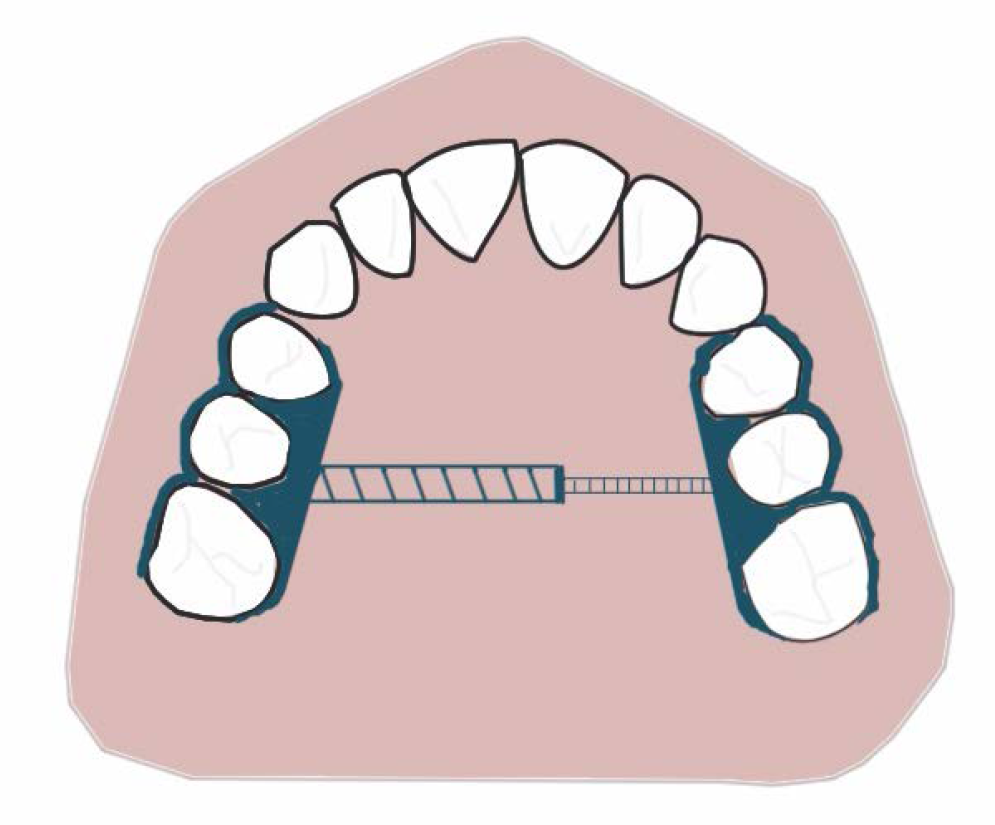
- Isaacson type of expansion.
7. Activation
In patient with 15 years of age 90 degree rotation can be activated twice in a day. In patients with above 50 years of age 45 degree activation is required 4 time/day. In older patient first 2 days should be two turns on each day followed by 1 turn/day for the 5-7 days and one time activation for alternative days till the acceptable amount of expansion is gained. The parent must be guided to active the screw for the younger patient. Mild pain may be felt during expansion1,9. [Figure 5(a) (b)]
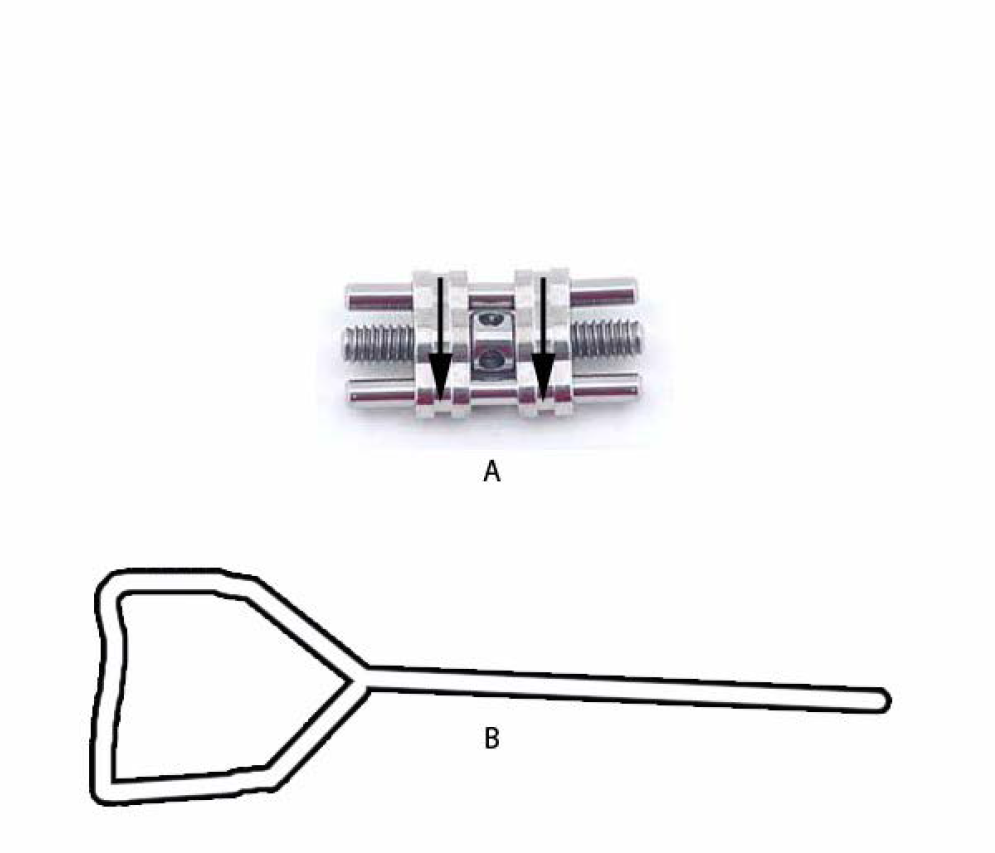
- (a) Typical expansion screw. (b) Key used for activation of appliance.
8. Conclusion
RME is more useful in several cases with moderate to severe discrepancy and maxillary construction and also used for increase the arch length. This procedure will improve nasal respiration and may be useful approach in dealing with abnormal breathing and OSAS. The appliance used in RME is more useful for expansion of the maxillary arch with limited duration. RME is a comparatively simple and conservative method of treatment.
References
- Rapid maxillary expansion and appliance an orthodontic solution for Obstructive Sleep Apnea Syndrome (OSAS) Sch J Dent Sci. 2016;3(1):1-3.
- [Google Scholar]
- Rapid maxillary expansion-A Review. Indian Journal of Orthodontics and Dentofacial Research. 2016;2(2):56-61.
- [Google Scholar]
- Rapid maxillary expansion: Unique treatment modality in dentistry. Journal of Clinical and Diagnostic Research. 2011;5(4):906-11.
- [Google Scholar]
- Maxillary expansion. Review article. International Journal of Clinical Pediatric Dentistry. 2010;3(3):139-46.
- [PubMed] [PubMed Central] [Google Scholar]
- Orthodontics exam preparatory manual for undergraduates (2nd ed). Elsevier; 2011. p. :443.
- [Google Scholar]




