
Translate this page into:
Early Childhood Dental Caries
-
Received: ,
Accepted: ,
This article was originally published by Informatics Publishing and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Every child needs a healthy smile. A healthy smile today can help protect overall health, encourage great dental habits, prevent future problems and even improve self-esteem of the budding torts.
Children are the most beautiful people on this earth. They are selfless and innocent. Their oral cavity is immensely clean, free of tartar and tobacco stains... You can mould the children as per your wish and one can shape them into good citizens of the country.
Oral health is a critical but an overlooked compo- nent of overall health and well-being among children and adults. Oral health problems such as dental caries, periodontal disease, and oral cancers are a global health problem in both industrialized and especially in devel- oping countries like India. Although there have been impressive advances in both dental technology and in the scientific understanding of oral diseases, significant disparities remain in both the rates of dental disease and access to dental care.
Dental caries is, undeniably, an international con- cern, especially amongst the pediatric population, being a somber public health problem. Dental caries in toddlers and infants has a distinctive pattern. Different names and terminology have been used to refer to the presence of dental caries among very young children. Early childhood tooth decay, early childhood caries, baby bottle tooth decay, early childhood dental decay, comforter caries, nursing caries, maxillary anterior caries, rampant caries, and many more. The term “early childhood caries” was suggested at a 1994 workshop organized by the Centers for Disease Control and Prevention, Atalanta USA in an attempt to focus attention on the multiple factors that contribute to caries at such early ages, rather than ascrib- ing sole causation to inappropriate feeding methods.
ECC is defined as “the presence of one or more decayed (noncavitated or cavitated lesions), missing teeth (due to caries), or filled tooth surfaces in any primary tooth in a child 72 of months age or younger.
Early childhood caries is predominantly a virulent form of dental caries, characterized by an overwhelm- ing infectious challenge and is associated with unusual dietary practices.
Despite the decline in the prevalence of dental caries in children in the western countries, caries in preschool children remains a problem in both developed and devel- oping countries like in our country.
As the disease progresses, decay appears on the occlu- sal surfaces of the primary maxillary first molars, with subsequent encroachment of other primary teeth, result- ing in the ultimate destruction of the primary dentition. Decay of primary teeth can affect children’s growth, lead- ing to malocclusion by adversely affecting the correct guidance of the permanent dentition. Children experi- encing caries as infants or toddlers have a much greater probability of subsequent caries in both the primary and permanent dentitions.
The classic etiology of ECC involves bacterial, dietary, and host determinants, which are influenced by the interplay of multiple sociological and environmental factors. The presence of cariogenic organisms, frequency of beverage and food consumption, oral hygiene status, parental education level, family income, caregivers’ oral health knowledge, maternal anxiety, and child temperament have all been shown to play roles in ECC (Figure 1).
- Etiology of dental caries.
The relationship between breast feeding and ECC is likely to be complex and confounded by many biological variables, such as mutans streptococci, enamel hypoplasia, intake of sugars, as well as social variables, which may affect oral health. More advanced technology that uti- lized chromosomal DNA patterns or identical plasmids provided more compelling evidence to substantiate the concept of vertical transmission. The investigations have shown that in children with ECC, S. mutans has regularly exceeded 30% of the cultivable plaque flora. In a normal predentate infant only the mucosal surfaces are exposed to salivary fluid flow. To persist in such an environment, S.mutans either forms adherent colonies on mucosal surfaces or live free in the saliva and duplicates at a rate exceeding the washout rate of salivary flow. The caries- associated microbiota in ECC becomes less diverse, perhaps because certain groups of microbes succeed or dominate the plaque biofilm as caries progresses.
The major reservoir from which infants acquire S. mutans is their mothers. In ECC, S.mutans strains iso- lated from mothers and their babies exhibits similar or identical bacteriocin profiles and identical plasmid or chromosomal DNA patterns. Successful colonization of infants by maternally transmitted S.mutans cells may be related to several factors, including magnitude of the inoculum, frequency of small-dose inoculations and minimum infective dose.
In young infants, this dental health care problem is associated with the frequent use of a baby bottle con- taining sweetened fluids with fermentable carbohydrates over extended periods, poor oral hygiene as well as a high level of mutans streptococci infection. This type of feeding behavior particularly during sleep intensifies the risk of early childhood caries, as oral clearance and salivary flow rate are decreased during sleep. Frequent intake of sugar in the form of liquids or solids leads to low pH conditions in the oral environment and in dental biofilm, favouring the growth of acidogenic and acidu- ric species. Moreover, sweetened liquids usually contain sucrose that is a specific substrate for glucan production, leading to adherence of mutans streptococci on the oral biofilm (Figures 2-4).
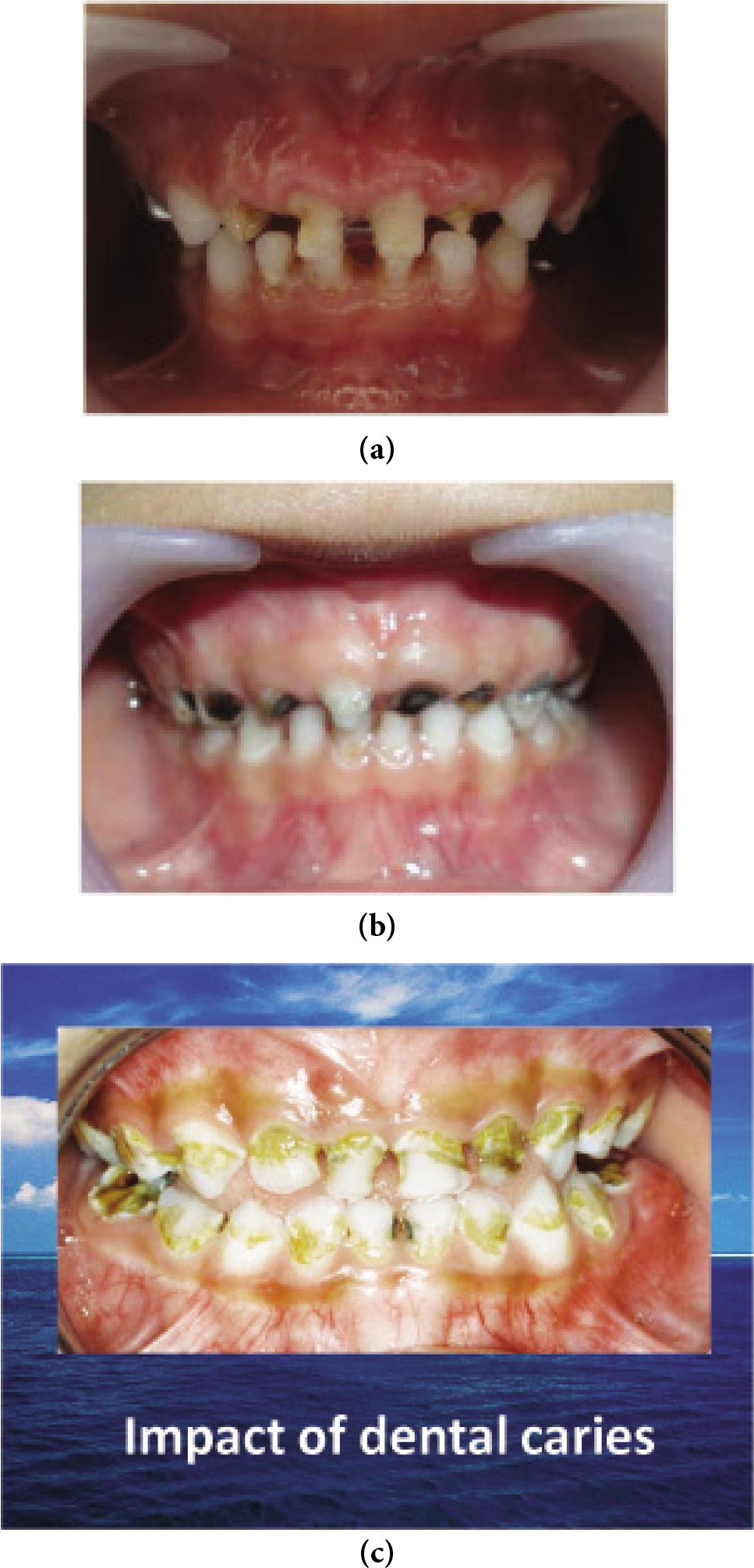
- (a)-(c) Adherence of mutans Streptococci on the oral Biofilm.
Unlike other infectious diseases, tooth decay is not self limiting. Therefore early diagnosis and early interven- tion is the key to its management as the children have the right to the enjoyment of the highest attainable standard of health, and to facilities for the treatment of illness and rehabilitation oh health.
Although largely preventable by early examination, identification of individual risk factors, parental coun- seling and education, and initiation of preventive care procedures such as topical fluoride application, the pro- gressive nature of dental disease can quickly diminish the general health and quality of life for the affected infants, toddlers, and children. Children’s quality of life can be seriously affected by severe caries because of pain and discomfort which could lead to disfigurement, acute and chronic infections, and altered eating and sleeping habits, as well as risk of hospitalization, high treatment costs, and loss of school days with the consequent diminished ability to learn.
The untreated severe caries with pulpitis affects growth, pulpitis and chronic dental abscesses affect growth by causing chronic inflammation that affects metabolic pathways where cytokines affect erythropoiesis. For example, interleukin 1 (IL1), which has a wide variety of actions in inflammation, can induce inhibition of erythropoiesis.
This suppression of hemoglobin can lead to anemia of chronic disease, as a result of depressed erythrocyte production in the bone marrow.
In light of the importance of perinatal oral health in preventing early childhood caries, and the need to intervene early for mother and child in a “dual parallel track” of treatment and disease prevention management, collaborations and partnerships among all health professionals are encouraged to foster early and timely oral health care and referrals for expectant mothers.
A promising approach toward primary prevention of ECC is to develop strategies that target the infectious component of this disease, for example by preventing or delaying primary acquisition of S.mutans at an early age through suppression of maternal reservoirs of the organism. Another approach is to prevent S.mutans from accumulating to pathologic levels through topical application of antimicrobial agents.
The expectant mother should be monitored for dental problems during pregnancy and given the appropriate prevention recommendations before the birth of baby. This is required to control the bacteria and eliminate the sources of infection, in view of the risk of bacterial transmission to the child.
Once the baby’s first tooth erupts, the child’s mouth must be cleaned with a wet cloth or with a child’s toothbrush and a small amount of fluoride toothpaste. Between the ages of 18 and 24 months, the child can learn to brush his teeth under adult supervision.
AMERICAN Academy of Pediatric Dentistry recommends that the Baby’s first dental visit should be during the first year of life, preferably during the first six months following the eruption of his first teeth, but no later than his first birthday Infant oral health visits should include caries risk assessment, individualized preventive strategies and anticipatory guidance.
A dual treatment plan approach is essential for moderate and high caries risk children and their parent/ caregivers. Strategies need to be employed to modify the maternal transmission of cariogenic bacteria to infants through the potential use of chlorhexidine rinse and xylitol products for caregivers, and fluoride varnish for both the caregiver and the child.
Additionally, the necessary changes in the child’s diet, toothbrushing, and fluoride application can be identified from the risk analysis. Expected parental compliance to recommended treatment protocols is essential for moderate and high caries risk children.
Parents should be given additional information and anticipatory guidance on the prevention of dental disease that is specific to the their child’s needs and caries risk factors, e.g., information on oral hygiene, growth and development, teething, digit or pacifier habits, oral habits, diet and nutrition, and injury prevention.
Pediatric dentists and general dentists have a critical role in preventing and reducing the Severity of early childhood caries. Caries risk assessment, individualized counseling, clinical preventive services such as fluoride varnish applications, xylitol use, and referral of high-risk infants and children to dental homes are increasingly being recognized as important elements of efforts to engage other pediatric health care providers in reducing the prevalence and severity of early childhood caries.
Summary
The Pediatric dentist, in particular, has many challenges to face and many queries and concerns to satisfy. The concept and role Pediatric Dentistry is still not a well understood phenomenon in the Indian population. The value of the child’s first dental visit is not very well heard of in this country. The child comes to visit the dentist only when the pain rocks and rolls his oral cavity. The concept of comprehensive care of the child’s oral cavity has not yet reached out to the masses of the country. The importance of teething, time of fluoride application, keeping a track of sequence and time of eruption, timely correction of the malocclusion, etc, needs to be globalized and nationalized.
Furthermore, a large junk of the Indian population falls below the poverty and the literacy line. This all renders the job of the Pediatric dentist and puts a halt in the way, dental care services could have been rendered to the people.
The caries process can be understood in very simple terms as being the result of acids generated by the dental biofilm from dietary fermentable carbohydrates causing demineralization of tooth mineral and ultimately leading to a caries lesion. However, the complex and dynamic environment created by interactions among dental biofilm, saliva, acquired pellicle, diet, and hard tissue itself must be taken into account to fully understand the caries disease process.




