
Translate this page into:
Case Report of Follicular Ameloblastoma-Extra(node)inary Presentation?
-
Received: ,
Accepted: ,
This article was originally published by Informatics Publishing and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Odontogenic tumours comprise of those neoplasms that arise from odontogenic cells and are restricted to the jaws which clinically manifest as swellings intraorally. Ameloblastoma is one of the odontogenic tumours which can be frequently seen affecting the mandibular third molar regions with an age range of 33 to 44 years. Here we present a case of Ameloblastoma which presented with its “textbook” intraoral presentation and radiographic features along with the unusual finding of single lymph node involvement which can elaborate the differential diagnosis to other tumours including malignant or aggressive transformation of a de novo tumor.
Keywords
Ameloblastoma
Odontogenic Tumors

1. Introduction
According to Robbins and Cotram (1979a) “A neoplasia is a new growth, comprising an abnormal collection of cells the growth of which exceeds and is uncoordinated with that of the normal tissue1”. Odontogenic cyst and tumors are diverse group of lesions that are observed predominantly in gnathic bones showing various clinical behaviours, histopathologic patterns varying from hamartamatous lesions, benign and malignant2. Odontogenic tumors are categorised fundamentally based on their origin from odontogenic ectomesenchyme and epithelium3. Ameloblastoma is the second most common tumor of odontogenic epithelium4. The exact origin of ameloblastoma is uncertain, but it is presumably due to transformation and mutation of genetic material in cells of odontogenic epithelium5. International Agency for Research on Cancer (IARC) and World Health Organisation (WHO) classified ameloblastoma into four subtypes namely, 1. Solid or multicystic ameloblastoma 2. Extraosseous or peripheral 3. Desmoplastic Ameloblastoma 4. Unicystic ameloblastoma6. Ameloblastoma can be asymptomatic for a period of 6 years or more,the symptom may be painless swelling of the jaw. Radiographically ameloblastoma is likely to be seen as unilocular or multilocular cyst like radiolucency with a radio-opaque border7. In this paper, we report a case of follicular ameloblastoma in a 17 year old male with emphasis on histopathologic findings and unusual presentation of lymphnode.
2. Case Report
A 17 year old male patient reported with a chief complaint of swelling in lower right back tooth region of the jaw for the past two months which gradually increased in size to its present size. No history of pain or pus discharge.
Extra oral examination showed a facial asymmetry on the right side. A diffuse oval swelling of 4 x 3 cm was seen on the right lower side of the face extending anteri-orly 4 cm from the corner of mouth and posteriorly to the angle of the mandible, superiorly to the ala-tragal line and inferiorly extending to the lower border of the mandible. Skin over the swelling was normal. On palpation, all the inspectory findings were confirmed, and the swelling was hard in consistency, with absence of tenderness. Right submandibular lymph node was palpable around 0.75 x 1 cm in size approximately, oval in shape, mobile, soft to firm in consistency and was tender on palpation (Figure 1).

- Extra oral photograph- large swelling in the lower right mandibular region.
Intra oral examination revealed a diffuse swelling of about 4 x 2 cm in size, irregular in shape, extending anteroposteriorly from 45 to 47, superiorly from the cervical region of 45 to 47 and inferiorly 1 cm above the right lingual sulcus of the mandible. On palpation, the swelling was soft in consistency on lingual side and hard in buccal side (Figure 2).

- Intra oral photograph- Intra oral swelling in the posterior aspect of mandible.
Orthopantomographic investigation revealed a multilocular radiolucency extending anteroposteriorly from 43 to 48, superiorly from alveolar ridge and inferiorly descending down to the lower border of the mandible. Also seen were, external resorption of roots of 45, 46, 47 (Figure 3). Computed Tomography (CT) had showed large round radiolucency in the posterior aspect of the mandible extending to the lower border of the mandible with thinning of the lingual cortical plate (Figure 4). The bicortical expansion was also clearly evident in the occlusal radiographic view supporting the diagnosis of odontogenic tumor (Figure 5).

- Panoramic radiograph- Large multi cystic radiolucencies extending to lower border of the mandible.

- Computed Tomography (CT)- Large radiolucency extending to lower border of the mandible.

- Occlusal radiograph.
With the above clinical and radiographic findings, a differential diagnosis of Odontogenic keratocyst and Ameloblastoma was made. An incisional biopsy was done under local anaesthesia and the specimen was sent for histopathological examination.
The microscopy showed an overlying parakeratinised stratified squamous epithelium of the oral mucosa in one area and numerous odontogenic epithelium in the form of small islands in the underlying connective tissue. These islands showed peripheral ameloblast like cells with central stellate reticulum like cells. Other areas exhibited fibrous connective tissue compressing odontogenic epithelium in the form of thin strands. Blood vessels and inflammatory cells were also observed in peripheral regions of the connective tissue. Since the section revealed predominantly a follicular pattern, a histopathologic diagnosis of Follicular type of Solid Multicystic Ameloblastoma was rendered (Figure 6 & 7). The histopathology of lymph node was negative for tumor cells as can be seen in Figure 8.
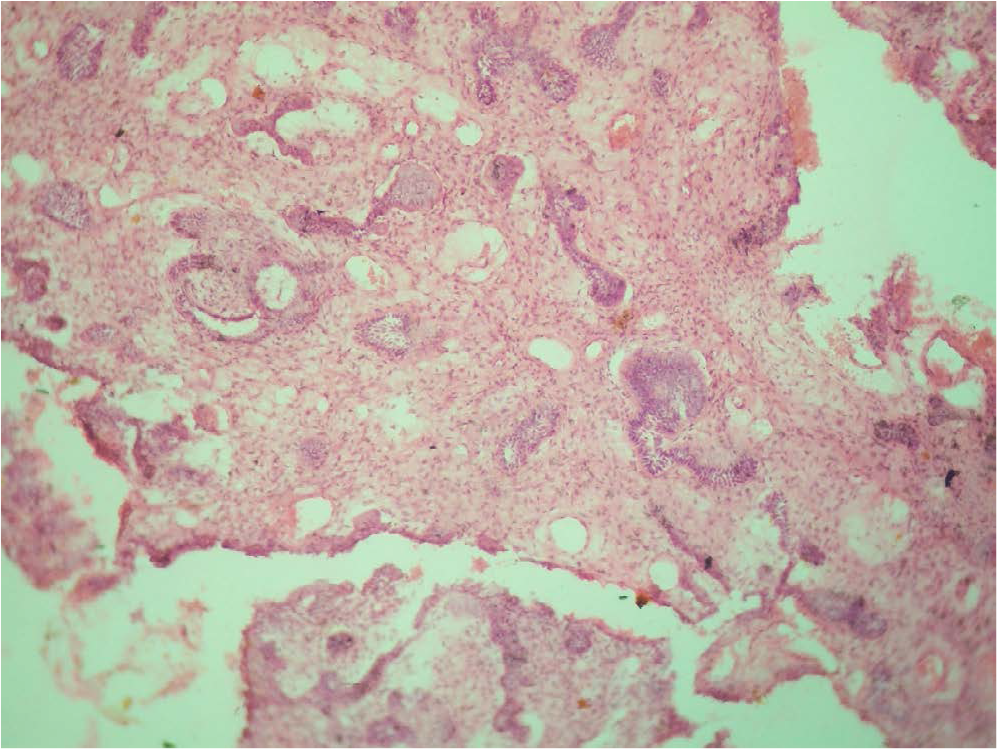
- Photomicrograph revealing odontogenic epithelial cells presenting a follicular pattern (10x).
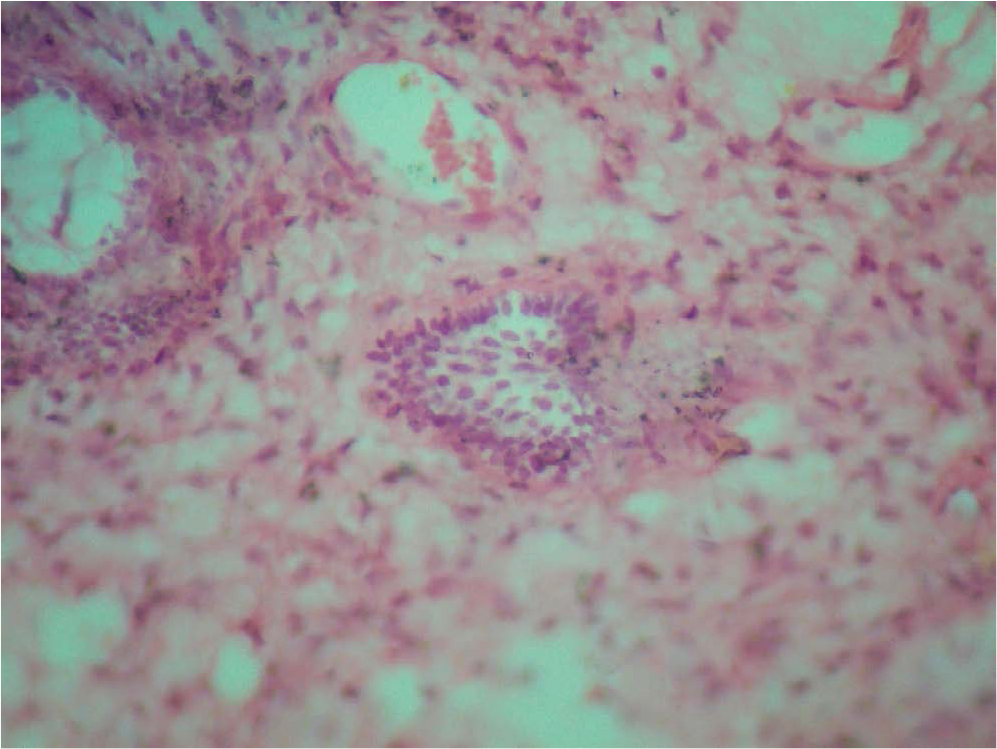
- Photomicrograph (40x)- High power showing a single ameloblastic follicle.
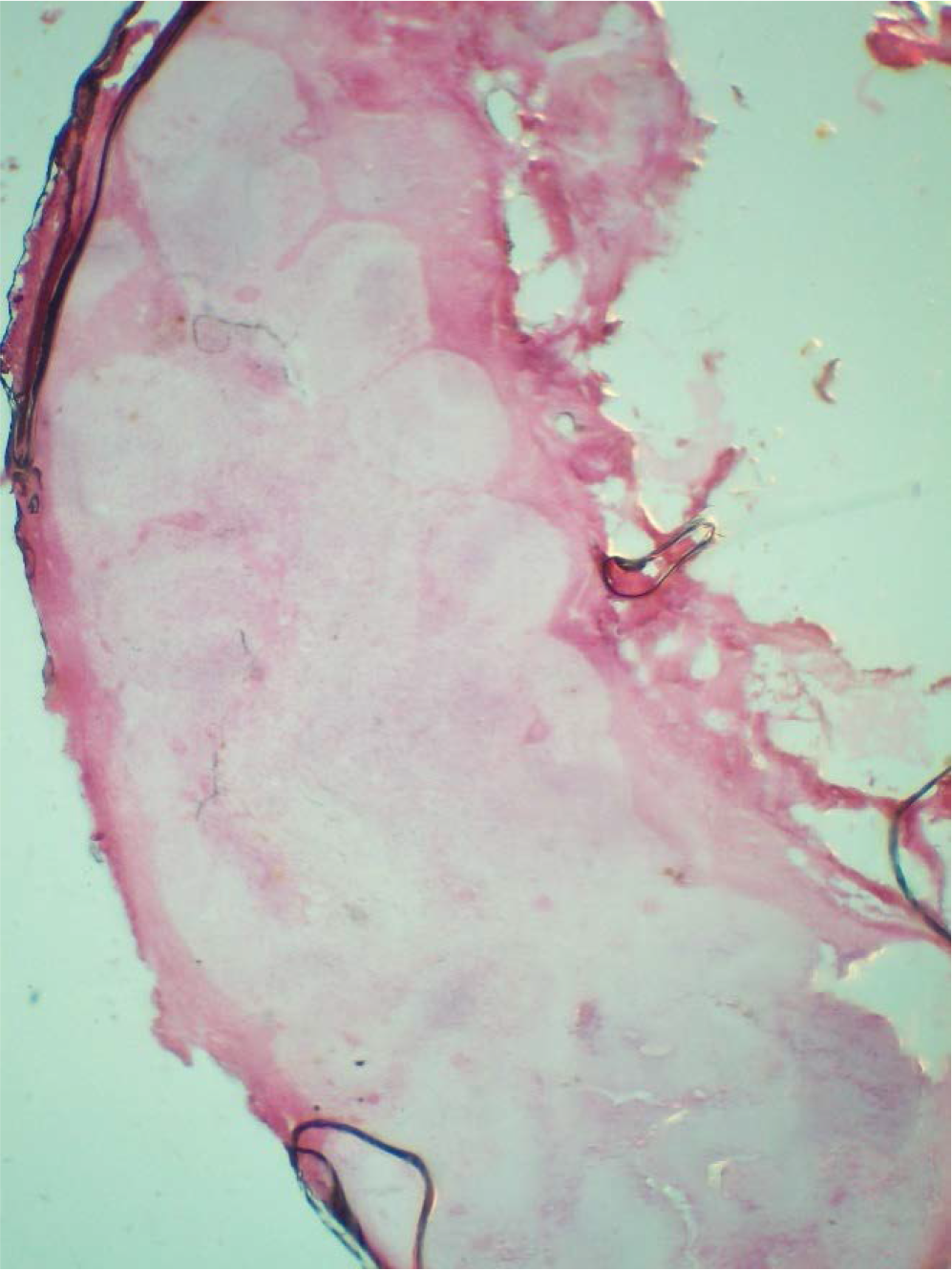
- Photomicrograph (4x)- Low power view showing the cross section of the suspicious lymphnode.
3. Discussion
The name Ameloblastoma was derived from a old French word “AMEL” and Greek word “BLASTOS” meaning Enamel and Germ/bud respectively8. Falkson was the first to give detailed description of ameloblastoma in 1879 but the term ameloblastoma was coined by Churchil in 1933. Over the past century this lesion was alluded to various names such as Cystosarcoma, Adamantinoma, Adamantine epithelioma, and lastly Ameloblastoma9. It is most commonly noted among 30 to 60 years of age10. Incidence is more common in males than in Females and they occur in both maxilla and mandible11. It is five times more common in molar region of mandible than in maxilla. Radiographically, they are seen as unilocular or multilocular radiolucent lesions with characteristic soap bubble or honey comb like appearance. Other features such as cortical plate expansion, thinning and erosion of cortex, resorption of adjacent roots and sometimes associated with displaced un-erupted tooth12. Histopathologically there are 6 subtypes based on pattern of arrangement of ameloblast like cells and stellate reticulum like cells of solid or multicystic ameloblastoma such as Follicular, Plexiform, Acanthomatous, Basal cell, Granular cell, and Desmoplastic. In an ameloblastic specimen various types of histological patterns can be observed, it is commonly classified based on the pattern that is predominant. Based on Vicker’s & Gorlin criteria the classic histologic feature of Ameloblastoma include darkly staining tall columnar cells with hyperchromatic nuclei in the periphery exhibiting palisading pattern and are also oriented away from basement membrane area of cell showing reversal of polarity. Stellate reticulum like cells placed in the centre of the island13.
In the present case, the clinical findings and radio-graphic features observed were suggestive of an odontogenic entity (tumor or cyst) except for the finding of single lymph node involvement hinting a “spread” or metastatic nature. The finding favouring a Ameloblastoma were the slow or gradually growing swelling in the posterior third region of the mandible along with bicortical expansion in a young patient of 17 years of age. The radio-graph, on the other hand, had showed large multiple cystic like radiolucencies in the posterior aspect of the mandible favouring an aggressive odontogenic keratocyst. Another atypical finding was the involvement of single lymphnode which was tender on palpation. The incisional biopsy showed the histopathology of follicular Ameloblastoma and the patient was referred to Oral Surgery for further treatment.
Categorizing ameloblastoma as whether they are benign or malignant has been a big debate because of its biological and histopathological properties. However in WHO, they clearly classify them as ameloblastoma, metastasizng ameloblastoma, ameloblasticcarcinoma14.
Nevertheless in this case follicular ameloblastoma was suspected to be a case of metastasizing ameloblastoma due to nodal involvement. But the excised lymph node was negative for tumor cells and showed only inflammatory cells suggesting reactive lymph node. Metastasizing ameloblastoma is seen in less than 2% of cases. Lung is the most common site for metastasis of about 75-80%, followed by cervical lymph nodes, diaphragm and brain15.
Generally metastatic spread of ameloblastoma occurs via blood, lymphatics or body fluids. However, Einsberg in her study hypothesized metastasis of ameloblastoma may be due to entrapment of odontogenic epithelium in lymphoid tissue during embryogenesis which may transform to benign tumor. This may be a second primary rather than metastasis to lymph node16.
Following the treatment of ameloblastoma long term follow up was always recommended because even after a very long disease free period cases were reported to have metastasis after treating the primary lesion. Disease free period may be even upto 42 years17.
References
- World Health Organization classification of tumours In: Pathology and genetics of head and neck tumours. Lyon: IARC Press; 2005. p. :435.
- [Google Scholar]
- WHO classification of Head and Neck Tumours In: Chapter 8: Odontogenic and maxilofacial bone tumours (4th ed). Lyon: IARC; 2017. p. :205-60.
- [Google Scholar]
- Hybrid ameloblastoma: Report of a rare case and review of literature. International Journal of Oral and Maxillofacial Pathology. 2011;2(4):68-72.
- [Google Scholar]
- Follicular ameloblastoma-a case report. Journal of Dental Sciences and Oral Rehabilitation 2011
- [Google Scholar]
- The need of a standardized surgical and pathological classification of tumors and anomalies of dental origin. Am Assoc Dent Sch Trans. 1930;7:240-5.
- [Google Scholar]
- Neuroophthalmologic aspects of ameloblastoma. Skull Base Surg. 1995;5(4):233-44.
- [CrossRef] [PubMed] [Google Scholar]
- Pathology of tumors of the oral tissues (4th ed). New York: Churchill Livingstone; 1984. p. :31.
- [Google Scholar]
- Radiologic and pathologic characteristics of benign and malignant lesions of the mandible. Radiographics. 2006;26:1751-68.
- [CrossRef] [PubMed] [Google Scholar]
- Odontogenic/ameloblastic carcinomas In: Barnes L, Everson JW, Reichart PA, Sidransky D, eds. World Health Organization classification of tumors, Pathology and genetics of head and neck tumors. Lyon: IARC press; 2005. p. :287-9.
- [Google Scholar]
- Malignant ameloblastoma: Concurrent presentation of primary and distant disease and review of the literature. J Oral Maxillofac Surg. 2012;70(10):2316-26.
- [CrossRef] [PubMed] [Google Scholar]
- Malignant (metastatic) ameloblastoma: Report of a case. J Oral Maxillofac Surg. 1993;51:1152-5.
- [CrossRef] [Google Scholar]
- Review of metastasizing (malignant) ameloblastoma (METAM): Pattern of metastasis and treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;111(6):734-41.
- [CrossRef] [PubMed] [Google Scholar]




