
Translate this page into:
Calcium and Inorganic Phosphorous Levels in Stimulated and Unstimulated Saliva in Early Childhood Caries – A Comparative Study
-
Received: ,
Accepted: ,
This article was originally published by Informatics Publishing and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction:
Saliva, a chief player in the oral cavity, is determined by its secretion rate and quality to aid either in the development of caries, or its remineralization.6 The ability for saliva to function as a source of calcium and phosphate increases its supportive properties as it influences the precipitation or dissolution of calcium hydroxyapatite (HAP), the principal inorganic component of dental hard tissue.
Materials & Methods:
30 healthy children, aged between 3 and 6 years old were screened and recruited for the study at the Department of Pedodontics and Preventive Dentistry of the A.B Shetty Memorial Institute of Dental Sciences, a constituent of Nitte University. The subjects were clinically examined and scored based on their decayed, missing (due to caries) and filled surfaces (dfs) and were further categorized into two equal groups of 15.
Result:
In the subjects with Early Childhood Caries (ECC), the mean calcium concentration in samples of unstimulated saliva was 4.2383 ± 0.8594 and in samples of stimulated saliva was 4.1965 ± 0.6240. While, the mean inorganic phosphorous concentration in samples of unstimulated saliva was 3.219 ± 0.8540and in samples of stimulated saliva was 3.0634 ± 0.5470.
Conclusion:
From this study, we obtained a relationship between calcium, saliva and the caries status of children with the calcium concentration decreasing with increase in the caries status, as well as on stimulation of saliva.
Keywords
Calcium
Phosphorous
Saliva
Stimulated

1. Introduction
Despite its global decline in the past decades, Early Childhood Caries (ECC) is still a significant problem in many developing countries and in a few developed nations1,2. The American Academy of Pediatric Dentistry (AAPD) was able to divide and classify early childhood caries depending on the age and number of Decayed, Missing or Filled tooth Surfaces (DMFS) in a child of less than 72 months of age. To be exact, the AAPD defines ECC as the presence of one or more decayed (non-cavitated or cavitated), missing (due to caries), or filled tooth surfaces in any primary tooth in a child 72 months of age or younger1. As children reach school age, they will have an increasing incidence of carious lesions because of change in dietary habits3 and due to other factors like oral hygiene, structure of the tooth, saliva and the presence of plaque4.
It is widely accepted through a number of studies5,6,7,8,9 that the etiology and pathogenesis of dental caries is multifactorial. Saliva, a chief player in the oral cavity, is determined by its secretion rate and quality to aid either in the development of caries, or its remineralization6. The lubricating and antimicrobial functions of saliva are maintained solely by this continuous flow of unstimulated saliva10. While on stimulation, protective properties increase such as salivary clearance, buffering power and degree of saturation with respect to tooth minerals such as calcium, phosphorous, and fluoride11. The ability for saliva to function as a source of calcium and phosphate increases its supportive properties as it influences the precipitation or dissolution of calcium hydroxyapatite (HAP), the principal inorganic component of dental hard tissue12.
There have been numerous studies7, 13,14,15 carried out to explore the relation between dental caries and flow rate of saliva when stimulated and unstimulated, as well as the level of concentrations of salivary constituents with the severity of caries12,16,17. However, this study combines the two, and focuses specifically on the vital tooth minerals, calcium and inorganic phosphorous, and the variation in its level in stimulated and unstimulated saliva of children suffering from Early Childhood Caries.
2. Materials & Methods
2.1 Sample Selection
30 healthy children, aged between 3 and 6 years old were screened and recruited for the study at the Department of Pedodontics and Preventive Dentistry of the A.B Shetty Memorial Institute of Dental Sciences, a constituent of Nitte University. Children who were taking any medication and or suffering from any systemic diseases were excluded from the study. The ethical clearance was obtained from the Institutional review board and the informed consent from the selectedstudy individuals.
The subjects were clinically examined and scored based on their decayed, missing (due to caries) and filled surfaces (dfs)18 and were further categorized into two equal groups of 15, as determined by American Academy of Pediatric Dentistry19 as shown in Table 1.
| AGE | EARLY CHILDHOOD CARIES GROUP | ||
|---|---|---|---|
| CF (dfs*) | ECC (dfs) | SECC (dfs) | |
| ≥36months (3 years) | 0 | 1 to 3 | ≥4 |
| ≥48months (4years) | 0 | 1 to 4 | ≥5 |
| ≤72 months (5-6 years) | 0 | 1 to 5 | ≥6 |
dfs – decayed (non-cavitated or cavitated lesions), missing (due to
caries) or filled tooth surfaces
CF – Caries –Free
ECC – Early Childhood Caries
SECC – Severe Early Childhood Caries
Group I: Early Childhood Caries
Group II: Control Group - Caries-Free
According to the AAPD19, children suffering from Early Childhood Caries were those with the presence of 1 or more decayed (non-cavitated or cavitated lesions), missing (due to caries), or filled tooth surfaces in any primary tooth in a child under 72 months of age.
2.2 Collection of Saliva
The subjects were instructed not to eat or drink anything for at least 1 hour before the collection of saliva sample. For the collection of unstimulated saliva, the subject was seated, head slightly down and was asked not to swallow or move his/her tongue or lips during the period of collection. The saliva was allowed to accumulate in the mouth for 2 minutes and then the subject was asked to expectorate the accumulated saliva into a clean, sterile, ice-chilled test tube.20
Immediately after this, for the collection of stimulated saliva, each subject was allowed to chew on a sterilized piece of rubber band on both sides of the jaw at a controlled rate for 2 minutes. Saliva collected during the first 10 seconds was discarded. The saliva was then allowed to accumulate in the mouth and the patient was asked to expectorate the accumulated saliva into a clean, sterile, ice-chilled test tube. This was continued till about 2-3mL of saliva was collected.20
The lid of the test tubes were closed immediately after collection and was stored at a temperature of 4°C while transported to the laboratory and at a temperature of 40°C until analysis20.
2.3 Laboratory Procedures–Salivary Analysis
Analysis of the samples was done on the same day. Samples were centrifuged at 5000 rpm for 5 minutes to remove debris9. Each sample was then estimated for calcium and phosphate concentrations. Estimation of these parameters was done by Autoanalyzer3,21,22(Ciba Corning, USA). Total calcium was estimated by using O-Cresolphthalein reagent22 and phosphorous concentration was estimated by using phosphomolybdate reagent22. These values were tabulated and subjected to statistical analysis.
2.4 Statistical Analysis
Student ‘t’ test was used to compare the mean values between stimulated and unstimulated saliva groups. P value of 0.05 or less was considered for standard significance.
3. Results
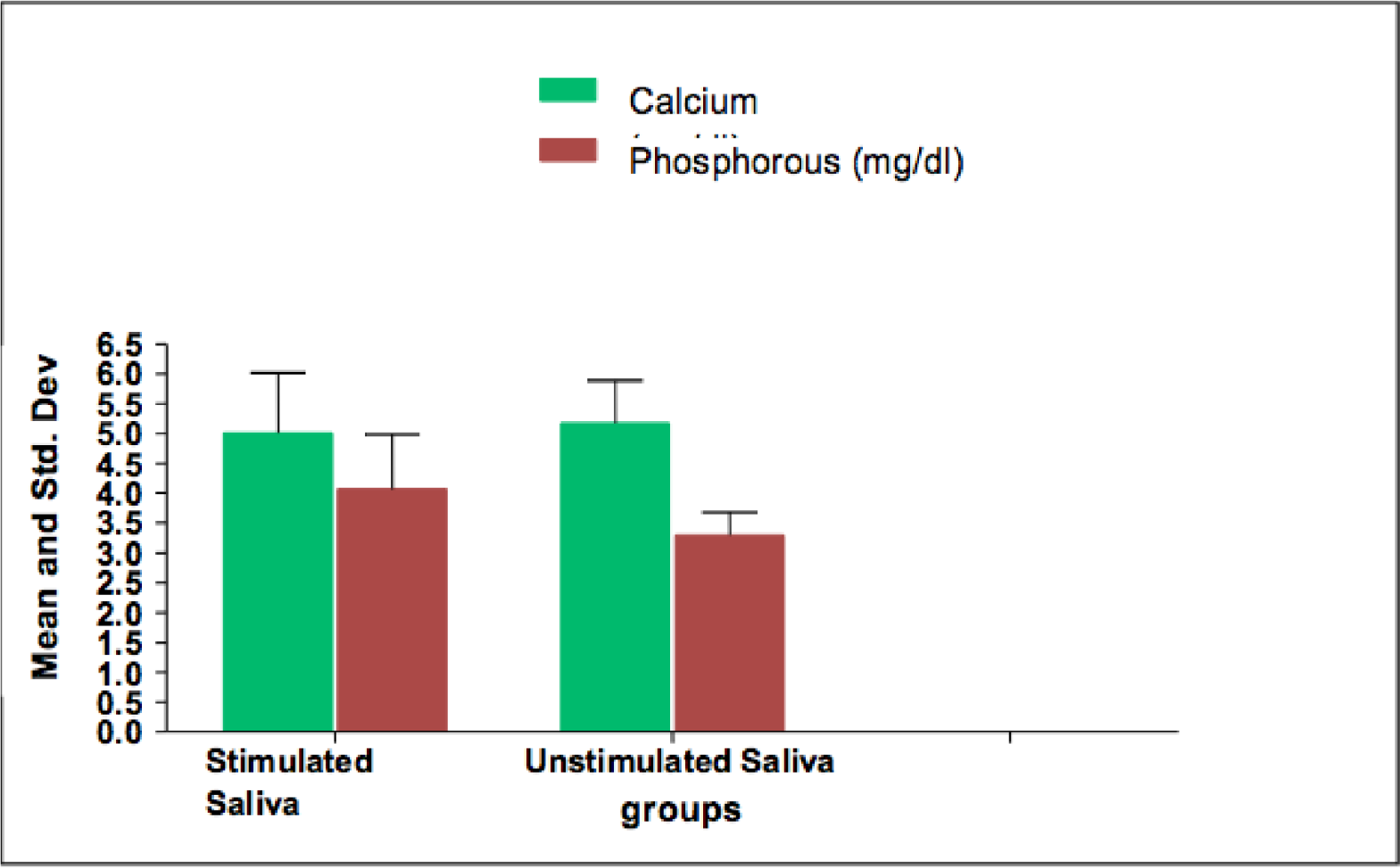
In the subjects with Early Childhood Caries (ECC), the mean calcium concentration in samples of unstimulated saliva was 4.2383 ± 0.8594 and in samples of stimulated saliva was 4.1965 ± 0.6240. While, the mean inorganic phosphorous concentration in samples of unstimulated saliva was 3.219 ± 0.8540and in samples of stimulated saliva was 3.0634 ± 0.5470.In Caries–Free (CF) subjects, the mean calcium concentration in samples of unstimulated saliva was 5.1732 ± 0.7136, while in stimulated saliva it was 5.01387 ± 1.0048. And the mean inorganic phosphorous level in samples of unstimulated saliva was3.29413 ± 0.3841 and in samples of stimulated saliva was 4.07175 ± 0.9117.
The calcium concentration levels were higher in unstimulated saliva than in stimulated saliva for both ECC and CF groups, but the difference was not statistically significant (P>0.05). Similarly, in the case of inorganic phosphorous, the levels were higher in unstimulated than stimulated saliva for the ECC group, proving to be not statistically significant (P>0.05). But, vice versa in the CF group, which was statistically significant when subjected to statistical analysis (P<0.05). However, when comparing both the calcium and inorganic phosphorous levels in saliva between the ECC and CF groups, the levels were higher in the CF subjects. This was proven to be statistically significant (P<0.05) except for the difference of phosphorous level in unstimulated saliva between the two groups.
Mean salivary calcium and phosphorous concentration values and their standard deviations of the test groups are exhibited in Figure 1 & 2. The results of the Student ‘t’ Test are shown in Table 2 & 3.

- Comparison of Means within Early Childhood Caries Group.
- Comparison of Means with Caries-Free Group.
| Calcium | SAMPLE COMPARISON VALUES (mean ± std. dev) | p-value | |
|---|---|---|---|
| GROUP | Stimulated Saliva (mg/dl) | Unstimulated Saliva (mg/dl) | |
| ECC | 4.1965 ± 0.62395 | 4.2383 ± 0.859406 | 0.9023 |
| Caries-Free | 5.01387 ± 1.004841 | 5.1732 ± 0.71355 | 0.688 |
| p-value | 0.05 | 0.025 | |
| Phosphorous | SAMPLE COMPARISON VALUES (mean ± std. dev) | p-value | |
|---|---|---|---|
| GROUP | Stimulated Saliva (mg/dl) | Unstimulated Saliva (mg/dl) | |
| ECC | 3.0634 ± 0.54696 | 3.219 ± 0.85389 | 0.633 |
| Caries-Free | 4.07175 ± 0.911698 | 3.29413 ± 0.384076 | 0.0286 |
| p-value | 0.01 | 0.810 | |
4. Discussion
Dental caries is a complex and dynamic process where a myriad of factors influence and initiate the progression of disease. Saliva, being a repository for many of these factors through its physiochemical properties --- such as pH, buffering capacity, salivary flow rate, concentration of various components like proteins, calcium and phosphorous --- plays a major role in the evolvement of dental caries23.
Central amongst the constituents of saliva, calcium and phosphorous, are most intimately related with the integrity of dental hard tissues24. From the moment of tooth eruption to the existence of the permanent dentition, the maturation of teeth through the diffusion of these ions into the surface enamel increases the surface hardness and resistance to caries25. Thus, an added cause for early childhood caries would be the deficiency in the salivary level of these ions during post-eruptive maturation.
According to the study of Anderson P. et al22, it was evaluated that the critical pH was lower in children than in adults, therefore making them more susceptible to caries since the thermodynamic forces for demineralization at low oral pH were greater. With this established, although a considerable amount of attention had been directed towards the calcium and phosphorous levels in saliva in relation to caries experience12,16,17,26 , the property of whether the saliva when stimulated or unstimulated has an effect on the levels of calcium and phosphorous has not been adequately supported, especially in the case of children. Along with this, the relationship between mildly reduced salivary flow and caries still remains less clear as described by the studies of Mandel13, Sreebny14, and Sweeney15.
Shannon et al27observed that the concentrations of calcium, phosphorous and magnesium in unstimulated saliva of the parotid gland are inversely related to flow rate in children with varied caries statuses. This study correlates with ours as calcium and inorganic phosphorous levels in the subjects with early childhood caries were higher in unstimulated saliva than in stimulated saliva by 0.5% and 2.5% respectively. The inverse relationship between the salivary flow rate and concentration of calcium and inorganic phosphorous was demonstrated, however when statistically proven, the difference was not significant (p>0.05).
When Caries-Free individuals were taken into consideration, the present study depicted an inverse relationship with the calcium level and salivary flow rate, with the concentration being greater in unstimulated saliva than stimulated saliva by 1.5%. Jonsgar28 had also estimated the calcium levels in resting and stimulated saliva in healthy individuals, causing similar results, as the flow of saliva increased in stimulated saliva, the calcium content decreased. In contrary to the effect of stimulation on the calcium level in saliva, the current study showed an increase in inorganic phosphorous concentration on stimulation of the saliva in Caries-Free subjects by 10.5%, proven to be statistically significant (p <0.05).This was disputed by studies of Patrick P. (2003)29, Clark TJ (2004)30, and Look M. P. et al31 who discovered that when comparing tests of stimulated saliva to unstimulated saliva, the calcium, magnesium as well as phosphate were significantly higher. On the other hand, studies of of Horton K. et al32 and Al-Zahawi S.M et al33 have found no correlation between phosphorous of saliva and dental caries, making this a controversial factor in the diagnosis of dental caries owing to it’s irregular pattern. Nevertheless, a suggestive cause for the significant increase of inorganic phosphorous on stimulation of saliva can be attributed to the breakdown of organic phosphatases by salivary phosphate enzymes resulting in increased occurrence of free phosphate ions. 34 This catabolic mechanism is more common in an alkaline environment which is directly associated with increased salivary flow, and further reflected in calculus formation35. With the additional parameter of calculus formation to define the relationship between increased inorganic phosphorous levels and increased salivary flow rates, the contradictory results of inorganic phosphorous in the stimulated saliva of Early Childhood Caries in the present study, could be owned to the inverse relationship of caries and calculus36. The above rationale can neither be established nor nullified without further studies and the additional parameter of general oral hygiene or calculus levels.
Shannon et al.37provided a basis upon which there is an increase in the calcium and phosphorous levels in unstimulated saliva (irrespective of the caries status) as the decrease in the rate of flow, increasingly concentrates the remaining constituents, such as calcium, phosphorous and magnesium and causes an inverse flow rate – constituent relationship. This enables the calcium and phosphate ions to accumulate in the saliva and either help in the enamel tooth maturation after eruption of teeth25or in the remineralization process which restores the stability of hydroxyapatite by replacing the missing ions in demineralized teeth38.
Moreover, when comparing the calcium and phosphorous levels in saliva between the subjects with Early Childhood Caries and Caries-Free subjects, the levels were mostly significantly higher in stimulated and unstimulated saliva of the Caries-Free individuals (p<0.05). Various studies 12,16,17,24 support the inverse relationship between calcium, inorganic phosphorous and the severity of caries. Shaw L. et al16, had attained results showing the mean levels of calcium and phosphorous in saliva and plaque to be significantly higher in caries-free than a high caries group. And Kittner D, Beetke E, and Kotzschke R.39examined similar results in the saliva of persons with a low caries experience.
With the calcium and inorganic phosphorous levels being more commonly increased in unstimulated saliva, as well as in subjects with lower caries statuses, several investigators40,41 proposed a solution – Calcium Phosphate containing chewing gums – which would increase the concentration of these elements in saliva that would promote the remineralizing properties of saliva in young subjects that are suffering from Early Childhood Caries or those more prone to caries. By using this gum, on stimulation of saliva, the level of calcium and phosphorous would be increased and would also supersaturate the saliva with these ions and inhibit demineralization of the tooth structure and remineralize early enamel lesions42.
The chief limitation of this study may be its small sample size. Thus, the results of this study is preliminary and further expansion of the study would extrapolate and strengthen the findings.
From this study, we obtained a relationship between calcium, saliva and the caries status of children with the calcium concentration decreasing with increase in the caries status, as well as on stimulation of saliva. However, inorganic phosphorous proved to be a volatile factor is diagnosing dental caries in children, with its inconsistent increase and decrease in concentration with respect to the caries status as well as flow rate of saliva. Further studies would reinforce the basis for this inference.
References
- Biological mechanisms of early childhood caries. Community Dent Oral Epidemiol. 1998;26:8-27.
- [Google Scholar]
- Risk indicators for early childhood caries Taiwan. Community Dent Oral Epidemiol. 2006;34:437-45.
- [Google Scholar]
- Relationship of Saliva and Plaque to Dental Caries. Journal of Dental Research. 1974;53:246.
- [Google Scholar]
- Understanding dental caries-Etiology and mechanisms, Basic and Clinical Aspects. . 1985;1:236-60.
- [Google Scholar]
- Identification of high caries risk adult: attitude, social factors and diseases. Int Dent J. 1988;38:231-80.
- [Google Scholar]
- Biological factors in dental caries: Role of Saliva and Dental Plaque in the Dynamic Process of Demineralization and Remineralization (part 1) J ClinPediatr Dent. 2003;28:47-52.
- [Google Scholar]
- Physical and Chemical Aspects of Saliva as Indicators of Risk for Dental Caries in human. J Dent Educ. 2001;65:1054-64.
- [Google Scholar]
- Secretion rate and buffer effect of resting and stimulated whole saliva as a function of age and sex. Swed Dent J. 1983;7:227-38.
- [Google Scholar]
- Relationship between calcium and inorganic phosphorus concentrations of both resting and stimulated saliva and dental plaque in children and young adults. Archives of Oral Biology. 1991;36:431-4.
- [Google Scholar]
- Salivary flow and dental caries In: I.D. Mandel, ed. Cariology today. Basel Kager; 1983. p. :56-69.
- [Google Scholar]
- Salivary flow and composition in relation to dental caries - methods and problems in studying this relationship in humans and animals In: I Kleinberg, S. Ellison, I. D. Mandel, eds. Saliva and dental caries 1979. New York Information Retrival Inc: New York; 1979.
- [Google Scholar]
- Calcium and phosphorus content of plaque and saliva in relation to dental caries. Caries Res. 1983;17:543-8.
- [Google Scholar]
- Salivary protein and some inorganic element levels in healthy children and their relationship to caries. J Marmara Univ Dent Fac. 1994;2(1):434-40.
- [Google Scholar]
- Studies on dental caries. I Dental status and dental needs of elementary school children. Public Health Rep. 1938;53:751. As quoted in Wilkins E.M.: Clinical Practice of The dental Hygienist. 8th ed. Philadelphia: Wolters Kluwer Company; 1999.293-313
- [Google Scholar]
- Diagnosing and reporting early childhood caries for research purposes. J Public Health Dent. 1999;59(3):192-7.
- [Google Scholar]
- FDI Working group 10 CORE; Saliva: Its role in health and disease. IDJ. 1992;42:291-304.
- [Google Scholar]
- Flow rate and composition of whole saliva in children from rural and urban Thailand with different caries prevalence and dietary intake. Caries Res. 1997;31:148-54.
- [Google Scholar]
- Critical pH in resting and stimulated whole saliva in groups of children and adults. Int J Paediatr Dent. 2001;11(4):266-73.
- [Google Scholar]
- Dental caries in the child and adolescent In: McDonald RE, Avery DR, Dean JA, eds. Dentistry for the child and adolescent (8th ed). St. Louis: Mosby Co; 2004. p. :203-5.
- [Google Scholar]
- Salivary Factors in Caries Prediction In: Methods of Caries Prediction. eds. Bibby B. G. and Shern R. J., Washington, D.C: Information Retrieval Inc; 1974. p. :147-58.
- [Google Scholar]
- Saliva and Its Relation to Oral Health Birmingham: University of Alabama Press; 1961.
- [Google Scholar]
- Inorganic Phosphate Concentration in Body Fluids as Related to Dental Caries. Status J Dent Res. 1962;41:1373-7.
- [Google Scholar]
- Comparison of salivary tests between unstimulated and stimulated saliva of children of different ages. Caries Res. 1986;20:153-4. Abstr.16
- [Google Scholar]
- The Relationship between Calcium, Magnesium, and Inorganic Phosphate of Human Mixed Saliva and Dental Caries. MDJ. 2007;4(2):157-61.
- [Google Scholar]
- Evidence for putting the calculus: caries inverse relationship to work. Community Dent Oral Epidemiol. 2005;33(5):349-56.
- [Google Scholar]
- Effect of Atropine-Induced Flow Rate Depression of the Composition of Unstimulated Parotid Fluid. Arch Oral Biol. 1969;14:761-70.
- [Google Scholar]
- Contents of phosphate and calcium in whole-saliva of test persons with high and low caries prevalence. Stomatol DDR. 1990;40(5):217-9. (Non English abstract.)
- [Google Scholar]
- Effects of calcium phosphates–containing chewing gums on whole saliva. J Dent Res. 1994;1:1314-5.
- [Google Scholar]
- Retention in Plaque and Remineralization of Enamel Lesions by Various Forms of Calcium in a Mouthrinse or Sugar-free Chewing Gum. J Dent Res. 2003;82:206.
- [Google Scholar]
- In vitro remineralisation of eroded enamel lesions by saliva. J Dent. 2001;29(5):371-6.
- [Google Scholar]




